MONTHLY FEATURE CPG SOPR SUMMARY
CPG Citation: Broder JS, Oliveira J E Silva L, Bellolio F, Freiermuth CE, Griffey RT, Hooker E, Jang TB, Meltzer AC, Mills AM, Pepper JD, Prakken SD, Repplinger MD, Upadhye S, Carpenter CR. Guidelines for Reasonable and Appropriate Care in the Emergency Department 2 (GRACE-2): Low-risk, recurrent abdominal pain in the emergency department. Acad Emerg Med. 2022 May; 29(5):526-560.
Downloadable at: Doi: 10.1111/acem.14495.
Scope of Guideline: CPG intended for ED physicians/clinicians who evaluate adult patients with Low-Risk Recurrent Abdominal Pain (LRRAP). Recs targeted for ED physicians in USA with access to advanced diagnostic imaging, lab tests and specialty referral.
Inclusion: Adult patients with multiple ED visits recurring over a period of months/years, with similar clinical presentations.

Summary download – click![]()
Exclusion: Children, adults with abnormal vital signs, clinical findings significant for acute abdominal pathology, or other risk factors for serious abdominal disease. Also not intended for new/acute presentations with a only short-term recurrence. Patients not previously evaluated for similar abdo pain in ED.
Key Words: Abdominal pain, analgesia, anxiety, computed tomography, depression, emergency department, low-risk, opioid, recurrent, ultrasound
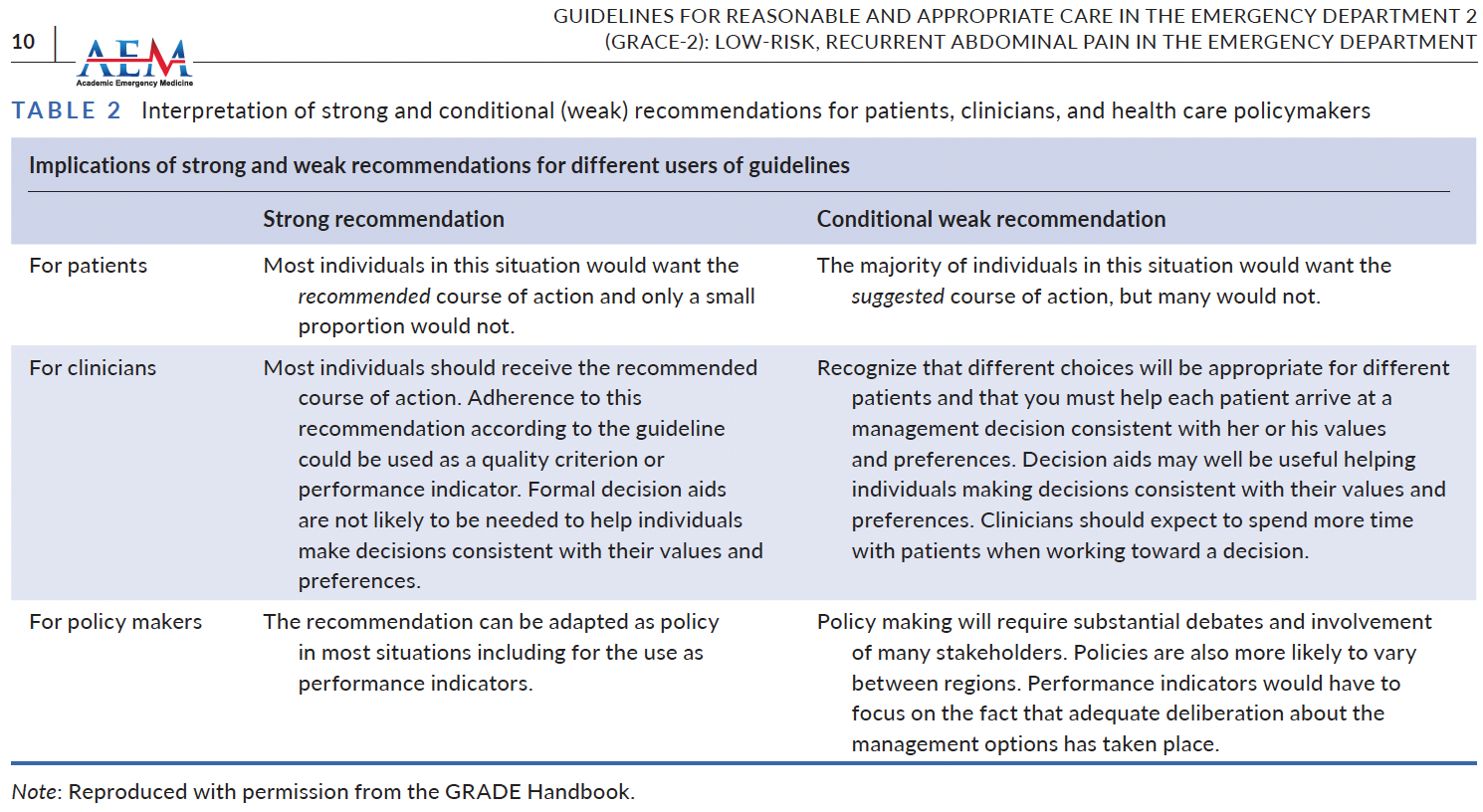
Key Recommendations: Each recommendation is accompanied by the “strength” of recommendation and the level of evidence (LoE) supporting that recommendation
| Recommendations (Strength, LoE) |
| Recommendation 1: In adult ED patients with low-risk, recurrent, undifferentiated abdominal pain and prior negative computed tomography of the abdomen and pelvis (CTAP) within 12 months, there is insufficient evidence to accurately identify populations in whom repeat imaging can be safely avoided or routinely recommended in the ED.(No recommendation) [No evidence] Recommendation 2: In adult ED patients with low-risk, recurrent, undifferentiated abdominal pain and a negative CTAP with IV contrast in the ED, we suggest against ultrasound unless there is concern for pelvic or biliary pathology. (Conditional recommendation, against) [Very low certainty of evidence] Recommendation 3: In adult ED patients with low-risk, recurrent, undifferentiated abdominal pain, we suggest screening for depression and/or anxiety may be performed during the ED evaluation. (Conditional recommendation, either) [Very low certainty of evidence] Recommendation 4: In adult ED patients with low-risk, recurrent, undifferentiated abdominal pain, we suggest an opioid-minimizing strategy for pain control. (Conditional recommendation, for) [Consensus, no evidence] |
Benefits of Recommendations: There is little evidence to guide decision-making re: repeat imaging in patients with LRRAP. Screening for depression/anxiety in LRRAP pateints may flag patients more suitable for psychiatric interventions, but there is no ED-based evidence to support this as a beneficial practice. A standardized approach to ED analgesia, ideally using standardized carepaths/algorithms, can increase equitable use of appropriate analgesia (ideally mechanistically based), and decrease the need for opioids during the ED stay and discharge. Newer analgesic agents (eg. ketamine) are also associated with less nausea/ vomiting problems usually associated with opioids. Finally, reducing the use of ED opioids can reduce any burden for long-term opioid misuse, which is beneficial in the ongoing opioid use crisis in North America and other parts of the world.
Harms/Adverse Effects of Recommendations: Approximately 90% of US exams after a negative CT will not add diagnostic value, and <1% will identify a surgical cause. There is a small but finite risk of radiation exposures (and subsequent cancers) that result from repeat CT scans. In a recent Canadian systematic review of inappropriate low-value care, it was found that diagnostic tests were inappropriately used approximately 28% of the time (Squires et al, CMAJ 2022; doi: 10.1503/cmaj.211416). Furthermore, repeat imaging during recurrent visits will increase costs (patient, system), length-of-stay, incidental findings that may result in future over-investigation and overdiagnosis, premature closure, and privacy concerns re: pelvic examinations for female patients. Screening for mood disorders can also result in overdiagnosis, low-value downstream referrals/treatments, and stigma concerns. It is not clear, also, how reliable the usual mood screening instruments (eg. Beck depression index, GAD-7 for anxiety) are in ED settings, and if their use has been validated in the ED. Furthermore, these instruments are time-consuming to complete, and require time/expertise to score them appropriately; this would, therefore, likely be a low priority in the ED.
Facilitators of Uptake: A shared decision-making process should be engaged with the patient with LRRAP, with a focus on the relative low yield of repeat imaging, and the incremental harms of repeat CT scans.
Barriers to Uptake: Lack of an evidence-based backstop to withhold recurrent imaging (US, CT) in LRRAP will likely result in ongoing over-imaging (over-diagnosis?) in the near future of ED practice. Lack of familiarity, time & expertise in the use of mood screening tools may restrict their application/implementation in ED settings. Finally, lack of familiarity/comfort with opioid analgesic alternatives may continue to drive opioid use in LRRAP (and other ED pain conditions), further exacerbating the ongoing opioid crisis.
CLINICAL COMMENTARY: LRRAP is a common and diagnostic resource-intensive/costly ED problem. Patients are often subjected to repeated imaging studies, and pain is treated invariably poorly. “Low-risk” criteria and other definitions outlined in Table 1.
A lot of low-value abdominal CT scans are done in the ED, without a resultant increase in diagnosed surgical disease, admissions or surgeries. Each CT adds a small but increased risk of cancer incidence over a lifetime. Adding an US after negative CT scan adds a new diagnosis in 10% of cases, no new surgical Dx, and adds considerably to ED LOS.
Depression/anxiety are common in ED LRRAP patients. Using a standardized screening scale (eg. PHQ-2 or -9 for depression, GAD-7 for anxiety) in the ED can detect these patients, who can then be referred to appropriate psychiatric services. A positive screen does not, however, help to rule out acute serious abdominal conditions, which should be evaluated as warranted during that ED visit. Screening may, however, be associated with overdiagnosis, false positives, leading to low-value psych referrals, investigations and treatments.
An opioid-sparing strategy is recommended as initial analgesia in LRRAP, especially in certain conditions (eg. renal colic, biliary colic). Use of standardized abdo pain carepaths can prioritize non-opioid analgesia first (and opioid rescue later), and optimize equitable treatment of pain. Avoiding opioid-induced nausea/vomiting with alternative analgesics is an attractive outcome for patients/providers. Analgesia equity is a serious problem for vulnerable populations (eg. women, elderly, non-Caucasians), and merits special attention in ED management.
There was no direct evidence to guide recommendations towards appropriate imaging practices for LRRAP. Clinical judgement should guide to consider different abdominal pathologies that may evolve at different rates, even with “normal” prior imaging/other testing.
It is important to maintain equitable care in assessing ED (LRRAP) concerns, in both diagnostic and analgesic interventions; 20% of Medicaid (vs. privately insured) patients, and 42-52% black/Hispanic patients (vs. white) were less likely to receive CT scans for LRRAP.
Prior Guideline Recommendations/Relevant Evidence: The evidence base (published in accompanying scoping & systematic reviews) is very thin and lacking direct evidence to inform GRADE tables for CPG Recs. Conditions explicitly addressed in other specialty CPGs (eg. surgery, urology, gastroenterology, OBGyne, etc.) also excluded.
Funding: Reported; funding by Society for Academic Emergency Medicine (SAEM) Guidelines for Reasonable and Appropriate Care in the Emergency Room (GRACE). Sponsor had no role in guideline design, evidence reviews and formulating Recs.
Conflicts of Interested: Reported; no conflicts declared by any panelists. **This Summary is created by one of the CPG authors.
Supporting References:
- Oliviera J. e Silva L, Prakken SD, Meltzer AC, Broder JS, Gerberi DJ, Upadhye S, Carpenter CR, Bellolio F. Depression and anxiety screening in emergency department patients with recurrent abdominal pain: An evidence synthesis for a clinical practice guideline. Acad Emerg Med 2021; PMID: 34665903 DOI: 10.1111/acem.14394.
- Carpenter CR, Griffey RT, Mills A, Doering M, Oliveira J eSilva L, Bellolio F, Upadhye S, Broder JS. Repeat computed tomography in recurrent abdominal pain: An evidence synthesis for guidelines for reasonable and appropriate care in the emergency department. Acad Emerg Med 2022; 29(5): 630-648. DOI: 10.1111/acem.1442
- Carpenter CR, e Silva LOJ, Upadhye S, Broder J, Bellolio F. A candle in the dark: The role of indirect evidence in emergency medicine clinical practice guidelines. Acad Emer Med 2022; DOI: 10.1111/acem.14494.

CPG Quality/ Trustworthiness Standards
Amalgamated from AGREE-II/NEATS instruments.
| Quality/Trustworthiness Domain | |
| The clinical practice guideline (CPG) discloses and states explicitly its funding source. | ✔ |
| Financial conflicts of interest of guideline development group (GDG) members have been disclosed and managed. | ✔ |
| The CPG development group includes all of the relevant multidisciplinary stakeholders, including clinicians, methodologists and patients/caregivers. | ✔ |
| The CPG objectives, health questions, scope of relevant providers and target recipients of care are clearly defined. | ✔ |
| Values/preferences of patients, caregivers, advocates and/or the public with experience with the clinical disease management has been sought/integrated into CPG development (reported clearly). | ✔ |
| The search strategy for evidence is thoroughly developed and described. | ✔ |
| The criteria for selecting relevant studies/evidence are clearly described. | ✔ |
| The quality, strengths and limitations of the body of evidence are clearly described (e.g., GRADE, Cochrane, etc.). Summaries of evidence tables are provided. | ✔ |
| The health benefits, side effects, and risks were considered in formulating the recommendations. | ✔ |
| There is an explicit approach linking the evidence to formulate the recommendations. | ✔ |
| The strength of recommendations is clearly reported, including confidence in underlying evidence. | ✔ |
| Recommendations are clear and unambiguous, and easily identified in the CPG publication. | ✔ |
| Different options for management for managing the health questions are clearly presented. | ✔ |
| Experts externally reviewed the guideline prior to its publication. | ✔ |
| The CPG describes a procedure to update the guideline, and provides advice, tools and/or clinical pathways for easy adoption/adaptation into practice. | X |
| The CPG describes barriers and facilitators to implement recommendations. | ✔ |
| Performance metrics for monitoring implementation of recommendations for audit/feedback have been defined appropriately. | X |
| Resource implications for implementing CPG recommendations have been discussed. | ✔ |