MONTHLY FEATURE CPG SOPR SUMMARY
CPG Citation: Gorelik M, Chung SA, Ardalan K, Binstadt BA, et al. 2021 American College of Rheumatology/Vasculitis Foundation Guideline for the Management of Kawasaki Disease. Arthritis Rheumatol. 2022 Apr;74(4): 586-596.
Downloadable at: doi: 10.1002/art.42041.
Scope of Guideline: Guideline aimed at providers who care for suspected KD/vasculitis patients.
Inclusion/Exclusion: Not clearly specified.
Key Words: Emergency department, IVIG, Kawasaki disease, unexplained fever, vasculitis
KEY RECOMMENDATIONS: Each recommendation is accompanied by the “strength” of recommendation and the level of evidence (LoE) supporting that recommendation

Summary download – click![]()
| Recommendations (ED-relevant) | Strength, LoE |
| Diagnostics: | |
| For children with suspected incomplete KD and fever, obtaining an echocardiogram with coronary artery measurements without delay is strongly recommended over not obtaining an echocardiogram. | Strong (Very Low) |
| For children with unexplained shock physiology, obtaining an echocardiogram with coronary artery measurements is strongly recommended. (Image coronary arteries also) | Strong (Very Low) |
| For children with unexplained MAS, obtaining an echocardiogram with coronary artery measurements is strongly recommended. | Strong (Very Low) |
| Therapeutics: | |
| For patients with incomplete KD, prompt treatment with IVIG at the time of diagnosis is strongly recommended over delaying treatment until day 10 or later. | Strong (Low) |
| For patients with acute KD and suspected or diagnosed MAS*, treatment with IVIG for KD and additional agents to treat MAS is strongly recommended. | Strong (Very Low) |
| For patients with acute KD, using aspirin is strongly recommended over no aspirin. | Strong (Very Low) |
| For patients with acute KD with subsequent resolution of fevers, continued daily monitoring for fevers is strongly recommended over not monitoring for fevers. | Strong (Very Low) |
| Therapeutics: | |
| For patients with acute KD who are at high risk of IVIG resistance or developing coronary artery aneurysms, use of IVIG with adjunctive glucocorticoids as initial therapy is conditionally recommended over treatment with IVIG alone. | Conditional (Low) |
| For patients with acute KD who are at high risk of IVIG resistance or developing coronary artery aneurysms, using IVIG with other nonglucocorticoid immunomodulatory immunosuppressive agents as initial therapy is conditionally recommended over treatment with IVIG alone. | Conditional (Very Low) |
| For patients with acute KD and persistent fevers after initial treatment with IVIG, a second course of IVIG is conditionally recommended over the use of glucocorticoids. | Conditional (Very Low) |
| For patients with acute KD who have arthritis that persists after IVIG treatment and who do not have coronary artery aneurysms, using NSAIDs to treat arthritis is conditionally recommended over not using NSAIDS. | Conditional (Very Low) |
| IVIG is the standard-of-care therapy for the initial treatment of KD. For patients with acute KD and persistent fevers after repeated treatment with IVIG, either nonglucocorticoid immunosuppressive therapy or glucocorticoids may be used. | Good Practice Statement (High)Ungraded Position Statement |
*MAS = Macrocyte Activation Syndrome; may be suspected in KD patients with persistent fever, splenomegaly, elevated ferritin levels, and thrombocytopenia.
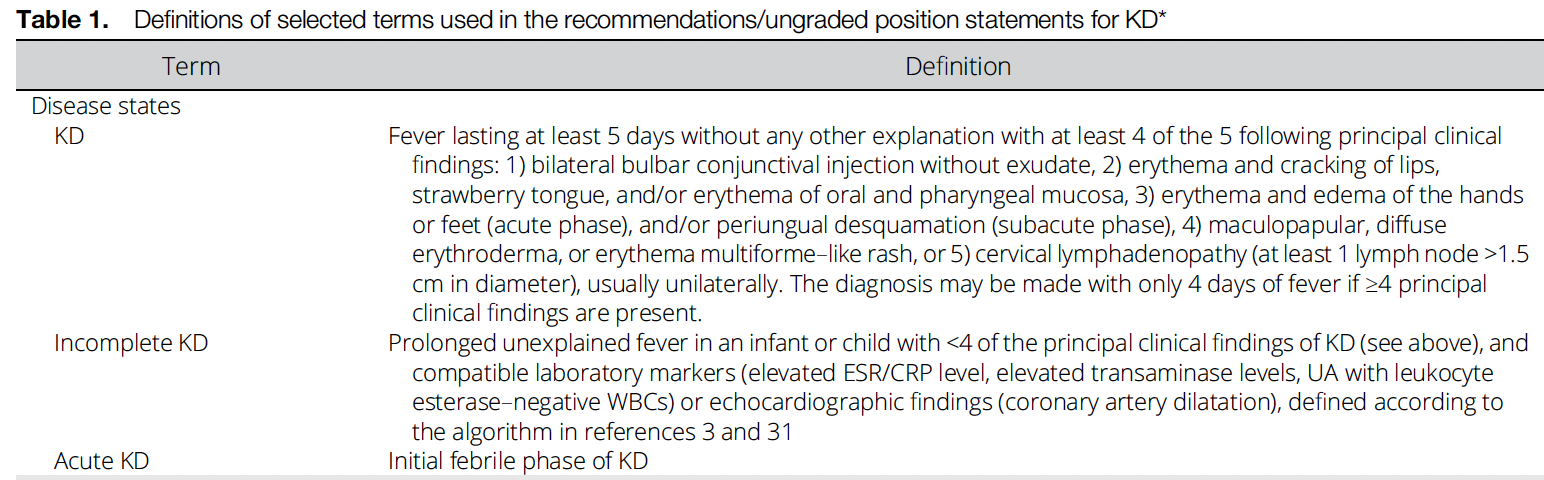
Benefits of Recommendations: Prior “major” and “minor” criteria for KD have been modified to KD and “incomplete KD” (see Table 1 below). This should be easily mastered by most EM physicians working in any ED setting. A broad (septic?) workup may be warranted for infants with prolonged FUO and clinical KD findings, including WBC counts, ESR, CRP and lactate levels. If evidence of splenomegaly, add ferritin levels and platelets to assess for possible MAS (see above).
A suspected diagnosis of KD should mandate an immediate referral/admission to pediatric specialists. In consultation with pediatric consultants, ED physicians should provide immediate aspirin treatment (reduce coronary inflammation and/or thrombosis), and arrange for IVIG infusion as expeditiously as possible. There is no evidence to recommend high dose ASA (80-100mg/kg/day) vs lower dose (3-5mg/kg/day). If there is high risk of potential coronary aneurysm formation (or ECHO evidence of aneurysms already), then adjunctive glucocorticoids can be administered with IVIG to reduce progression. (Risk prediction scores for aneurysm risk are not historically very reliable?). Typical steroid dose of prednisone = 2mg/kg/day (max 60mg/day). Other immunomodulary agents (eg. infliximab, anakinra, cyclosporine) treatments can likely be deferred to admitting specialists.
Harms/Adverse Effects of Recommendations: KD can be an easily missed diagnosis if not specifically investigated in the ED setting in the context of prolonged FUO patients (esp 5+ days). The potential outcomes of missed KD are significant for cardiac complications.
There is little downside to giving immediate aspirin (3-5mg/kg/day) in the ED, and discussing IVIG initiation with pediatric consultants pending transfer/admission.
Facilitators of Uptake: Included clinical carepath can be adapted for ED usage, with an emphasis on enhanced recognition and diagnostic testing for KD/MAS clinical features.
Barriers to Uptake: Missed diagnosis in ED patients with prolonged FUO.
CLINICAL COMMENTARY: Kawasaki disease (KD) is a common pediatric vasculitis, with an incidence of 25-50cases/100K children annually in USA. It is the most common cause of acquired heart disease in childhood, with 25% untreated children getting coronary aneurysms if left untreated (50% infants <6mo). Accurate diagnosis and early treatment is critical to reduce this risk.
Prior Guideline Recommendations/Relevant Evidence: These Recs build on prior guidance, and updates definitions of KD to be more practical (Yellen et al 2010, McCrindle et al 2017).
Funding: Reported. Funding from American College of Rheumatology & Vasculitis Foundation.
Conflicts of Interested: Reported; minimal (online Supp materials)

CPG Quality/ Trustworthiness Standards Amalgamated from AGREE-II/NEATS instruments
| Quality/Trustworthiness Domain | |
| The clinical practice guideline (CPG) discloses and states explicitly its funding source. | ✔ |
| Financial conflicts of interest of guideline development group (GDG) members have been disclosed and managed. | ✔ |
| The CPG development group includes all of the relevant multidisciplinary stakeholders, including clinicians, methodologists and patients/caregivers. | ✔ |
| The CPG objectives, health questions, scope of relevant providers and target recipients of care are clearly defined. | ✔ |
| Values/preferences of patients, caregivers, advocates and/or the public with experience with the clinical disease management has been sought/integrated into CPG development (reported clearly). | ✔ |
| The search strategy for evidence is thoroughly developed and described. | ✔ |
| The criteria for selecting relevant studies/evidence are clearly described. | ✔ |
| The quality, strengths and limitations of the body of evidence are clearly described (e.g., GRADE, Cochrane, etc.). Summaries of evidence tables are provided. | ✔ |
| The health benefits, side effects, and risks were considered in formulating the recommendations. | ? |
| There is an explicit approach linking the evidence to formulate the recommendations. | ✔ |
| The strength of recommendations is clearly reported, including confidence in underlying evidence. | ✔ |
| Recommendations are clear and unambiguous, and easily identified in the CPG publication. | ✔ |
| Different options for management for managing the health questions are clearly presented. | X |
| Experts externally reviewed the guideline prior to its publication. | X |
| The CPG describes a procedure to update the guideline, and provides advice, tools and/or clinical pathways for easy adoption/adaptation into practice. | ? |
| The CPG describes barriers and facilitators to implement recommendations. | X |
| Performance metrics for monitoring implementation of recommendations for audit/feedback have been defined appropriately. | X |
| Resource implications for implementing CPG recommendations have been discussed. | X |