MONTHLY FEATURE CPG SOPR SUMMARY – October 2022
CPG Citation: VA/DoD Clinical Practice Guideline. (2022). The Diagnosis and Treatment of Low Back Pain. Washington, DC: U.S. Government Printing Office.
Downloadable at: VA DoD https://www.healthquality.va.gov/guidelines/pain/lbp/
Scope of Guideline: Providers who care for low back pain.
Inclusion: Adults (ages 18 years or older) with acute, subacute, or chronic LBP with or without neurological symptoms.
Exclusion: Patients with known cancer, infections, inflammatory arthropathies, visceral disorders, pregnant women.

Summary download – click![]()
Key Words: Back pain, guideline, red flags.
Key Recommendations: (STRONG/Neither/Weak) ED-Relevant
Clinical Action FOR
- We recommend the history and physical examination include evaluation for progressive or otherwise serious neurologic deficits and other red flags (e.g., signs, symptoms, history) associated with serious underlying pathology (e.g., malignancy, fracture, infection); STRONG
- We recommend diagnostic imaging and appropriate laboratory testing when neurologic deficits are progressive or otherwise serious or when other red flags (e.g., signs, symptoms, history) are present; STRONG
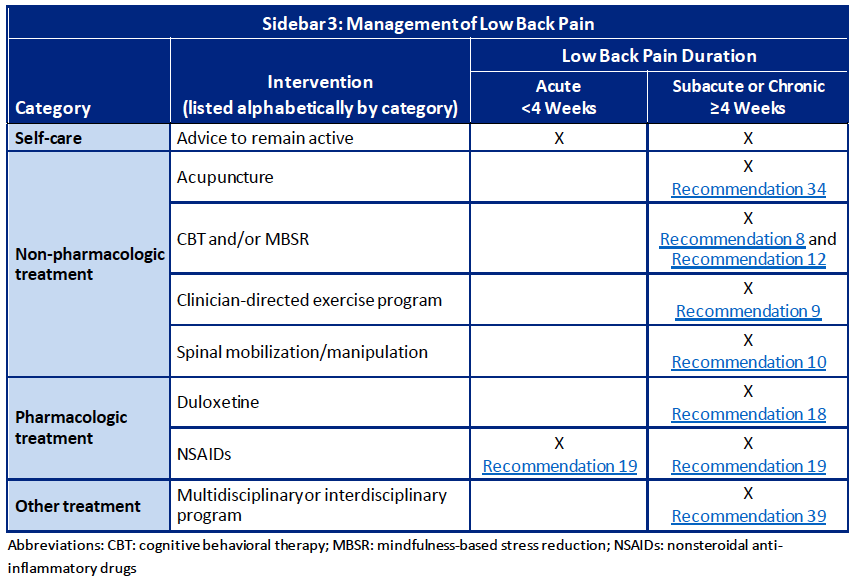
- For patients with chronic low back pain, we suggest duloxetine; WEAK
- For patients with low back pain, we suggest nonsteroidal anti-inflammatory drugs; WEAK
- For patients with chronic low back pain, we suggest lumbar medial branch and/or sacral lateral branch radiofrequency ablation. WEAK
- For patients with chronic low back pain, we suggest acupuncture. WEAK
- For patients with chronic low back pain, we suggest a multidisciplinary or interdisciplinary program. These programs should include at least one physical component and at least one other component of the biopsychosocial model (psychological, social, and/or occupational) used in an explicitly coordinated manner. WEAK
NEUTRAL Clinical Action (Weak For or Against, or Neither)
- We suggest assessing psychosocial factors and using predictive screening instruments (e.g., STarT Back and The Orebro Musculoskeletal Pain Screening Questionnaire) to inform treatment planning (Weak For).
- For patients with low back pain, with or without radicular symptoms, there is insufficient evidence to recommend for or against specific physical exam maneuvers to assist in the diagnosis of facet or sacroiliac joint pain, or a lumbar/lumbo-sacral radiculopathy (Neither).
- There is insufficient evidence to recommend for or against pain neuroscience education, clinician-directed education with patient-led goal setting, or back school (Neither).
- For the self-management of low back pain, there is insufficient evidence to recommend for or against technology-based modalities (Neither).
- For patients with chronic low back pain, we suggest cognitive behavioral therapy (Weak For).
- For patients with any low back pain, we suggest a structured clinician-directed exercise program (e.g., aerobic, aquatic, mechanical diagnosis and therapy, mobility, motor control, Pilates, strengthening exercises, structured walking program, tai chi). (Weak For).
- For patients with chronic low back pain, we suggest spinal mobilization/manipulation (Weak For).
- For patients with acute low back pain, there is insufficient evidence to recommend for or against spinal mobilization/manipulation (Neither).
- For patients with chronic low back pain, there is insufficient evidence to recommend for or against mindfulness-based stress reduction (Neither).
- For patients with low back pain, there is insufficient evidence to recommend for or against lumbar supports, or mechanical lumbar traction (Neither x 2).
- For patients with chronic low back pain, there is insufficient evidence to recommend for or against auricular acupressure, cupping, laser Rx, TENS or US therapies (Neither for all).
- For patients with low back pain, there is insufficient evidence to recommend for or against yoga or qi gong (Neither).
- For patients with low back pain, with or without radicular symptoms, there is insufficient evidence to recommend for or against gabapentin or pregabalin, tricyclic antidepressants or topical agents (Neither for all).
- For patients with acute low back pain, there is insufficient evidence to recommend for or against a non-benzodiazepine muscle relaxant for short-term use (Neither).
- For patients with low back pain, there is insufficient evidence to recommend for or against any specific diet or nutritional, herbal, or homeopathic supplements (e.g., anti-inflammatory diet, turmeric, vitamin D), cannabis, or cannabinoids (Neither).
- For patients with low back pain, there is insufficient evidence to recommend for or against sacroiliac joint injections (Neither).
- For patients with acute low back pain, there is insufficient evidence to recommend for or against acupuncture (Neither).
- For patients with low back pain, there is insufficient evidence to recommend for or against ortho-biologics (e.g., platelet-rich plasma, stem cells); Neither.
- For patients with low back pain, with radicular symptoms, there is insufficient evidence to recommend for or against epidural steroid injections (Neither).
Clinical Action AGAINST
- For patients with acute low back pain, without focal neurologic deficits or other red flags (e.g., signs, symptoms, history), we recommend against routinely obtaining imaging studies or performing invasive diagnostic tests; STRONG.
- For patients with chronic low back pain, we suggest against offering a non-benzodiazepine muscle relaxant, acetaminophen, and monoclonal antibodies (Weak for all).
- For patients with chronic low back pain, we suggest against opioids. For patients who are already using long-term opioids, see the VA/DoD CPG for the Use of Opioids in the Management of Chronic Pain (Weak). Consult your local opioid prescribing guidelines (provincial, national).
- For patients with low back pain, with or without radicular symptoms, we suggest against systemic corticosteroids (oral or intramuscular injection); (Weak).
- For patients with low back pain, we recommend against benzodiazepines (STRONG).
- For patients with low back pain, we suggest against the injection of corticosteroids for intra-articular facet joint injections and therapeutic medial branch blocks with steroid (WEAK).
- For patients with low back pain, we suggest against spinal cord stimulation (WEAK).
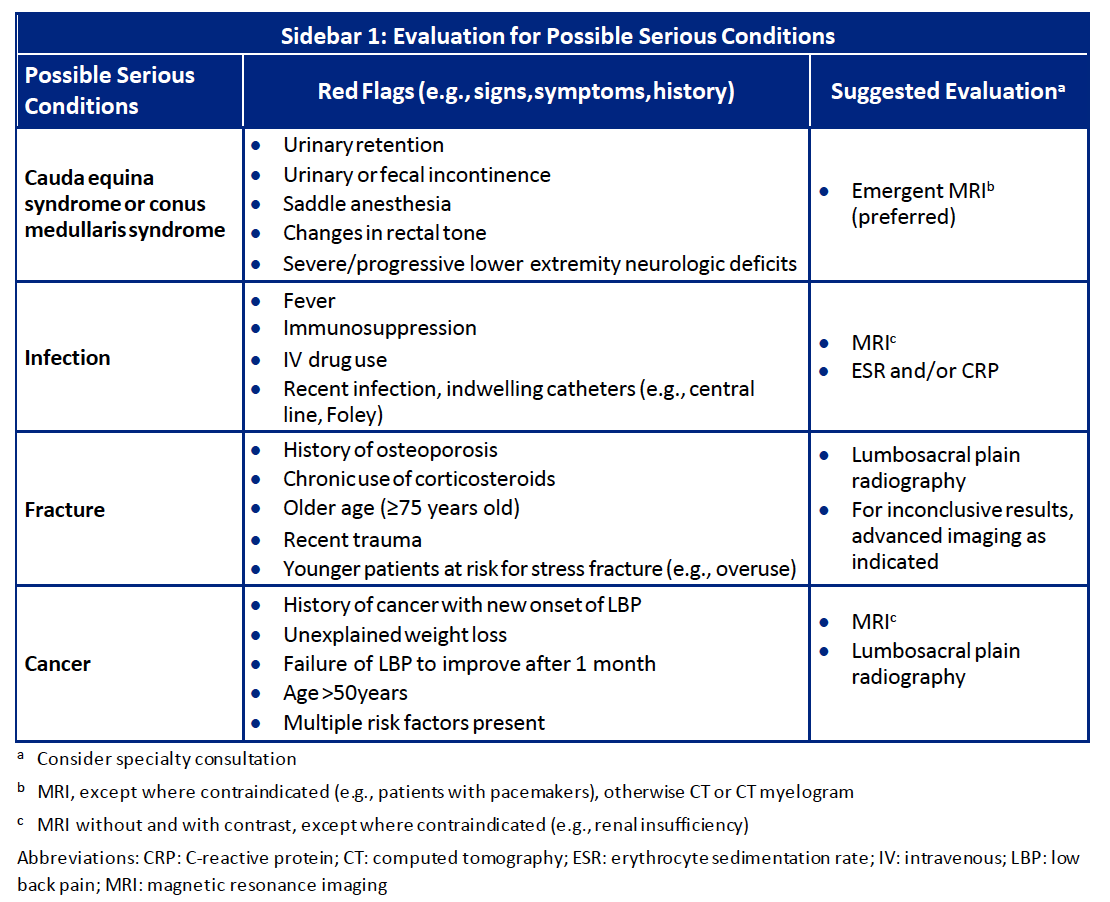
CLINICAL COMMENTARY: Low back pain in the ED is a very common complaint, and serious pathologies are rare (x%). Nonetheless, a standardized approach to ruling out “red flag” serious pathologies (“NIFTI” = Neurologic, Infection, Fracture, Tumour, Inflammation) is critical to ensure no serious diagnostic misses. Regrettably, clinical assessment of red flags has variable diagnostic test utility, with moderate quality evidence supporting assessment for the likelihood of malignancy and fracture, and low-quality evidence for spinal epidural abscess. A recent systematic review of ED low back pain red flags is summarized below (Galliker et al, 2020):
- For detection of epidural abscess, there was an increased risk in patients with a history of intravenous (IV) drug use and other infection sites (likelihood ratio [LR]+:13.7), an indwelling vascular catheter (LR+: 15.7), or a history of recent spine fracture (LR+: 9.5). Regrettably, 50% patients will be afebrile and/or no neurologic deficits, which may lead to diagnostic (ie. imaging) delay. The “classic triad” of back pain, unexplained fever, and abnormal labs (WBC, ESR) are only present in <15% of ED LBP patients.
- For detection of vertebral fracture, there was a large risk with a history of trauma with neurological findings on physical examination (LR+: 31.1). Another study of 700pts suggested the following risk factors for vertebral fracture: older age >75yo, recent trauma, osteoporosis, severe back pain (score >7/10), and thoracic pain. Physical findings of contusion/abrasion has a strong predictive likelihood (LR+ 31.1; Upadhye et al, 2016). The presence of multiple findings may increase risk of fracture to 42-90%.
- For detection of cancer-causing LBP, there was a large risk with a combination of a history of cancer and the clinical suspicion of cancer (LR+: 27.9). History of malignancy is associated with a higher risk of identifying serious underlying causes of LBP. In patients with unexplained weight loss, failure to improve after one month, or age greater than 50 years, the likelihood of cancer as the cause of LBP increased to approximately 1.2%.
- For detection of spinal compression/cauda equina syndrome (CES), these include the above red flags, and use of oral anticoagulants (OACs) that may lead to insidious/acute hematoma. Use of OACs may also be associated with acute abdominal mimicks of low back pain (eg. retroperitoneal bleeds, AAA/dissections, etc.).
Benefits of Recommendations: This guideline is methodologically very strong, and meets nearly all AGREE-II/NEATS trustworthiness standards. The details of the GRADE literature reviews and formulation of recommendations are reliable and transparent.
For ED practice, there is useful information provided with respect to assessing potential “red flags” that warrant further investigations/labs/referral in the ED. There is an algorithm with associated Sidebars that can inform ED management. Acute analgesia usually starts with NSAIDs (assuming no contraindications), followed by specific agents for neuropathic pain as needed, and possibly a short course of cannabinoids/opioids to avoid any short-term sensitization concerns. Reinforcement to encourage early mobilization after acute injury is also presented.
Of note, early imaging for non-emergent conditions is NOT recommended, and has been associated with with worse clinical outcomes. These include early unnecessary surgeries, higher overall costs/healthcare utilization, loss of work, and potential opioid over-use/disorders (Jacobs et al, 2020; Lemmers et al 2019).
Harms/Adverse Effects of Recommendations: There is a potential conflict with the Rec to not investigate non-serious pathologies in the ED, since they may run contrary to patient preferences to have a confirmatory diagnosis (including low-value ED imaging). The Patient Panel did have significant inputs, however, in framing this Rec in order to obviate any conflicts/complaints in the ED.
There are no specific directional Recs re: mobilization after acute/chronic pain, since the evidence is weak and mixed on benefits of different modalities. There is, however, indirect evidence that early mobilization after acute back injury is key to earlier recovery, and that participation in active modalities (eg. physiotherapy, yoga, Taichi, pilates, aquafit) are superior to passive (eg. massage, chiropractic, acupuncture, laser, US, heat/cold, TENS, etc). This was recently confirmed in a randomized trial (Peng et al, 2022).
Barriers to Uptake: This CPG is primarily aimed at primary care/outpatient practices, but contains relevant information for ED practice also. Assessing for psychosocial “yellow” flags may not be practical in the ED, given time restraints and uncertain validity of screening tools in ED populations. Physical exam maneuvres may have variable diagnostic utility in the ED setting, and may/may not contribute to choices regarding further investigations, especially with different levels of training/expertise in such specific maneuvres. Generally, they lack sufficient sensitivity to “rule out” serious pathologies, and the body of supporting evidence is rather low quality.
Facilitators of Uptake: There are some clinical algorithms that could be adapted for ED usage (Algorithm Module A, pg 18). Recommended (ED?) imaging modalities for Serious Pathologies are listed in Sidebar 1 (see below). Investigations for other less urgent back diagnoses are listed in Sidebar 2.
There are no comments about use of minor interventional pain procedures (eg. nerve blocks, trigger point/bursa/ligament/tendon complex/joint injections) in ED patients with mechanical low back pain (ie. no red flags), but there are some external reports about the utility of such to get faster pain relief in the ED, and mobilize patients for discharge quicker than traditional enteral/parenteral analgesics used. This is an area that merits further exploration…
Prior Guideline Recommendations/Relevant Evidence: This is an extension/update of the 2017 VA/DoD LBP CPG.
Recent 2021 updates for the Appropriateness Criteria of imaging for low back pain (including emergent conditions) are published by the American College of Radiology (downloadable at: https://acsearch.acr.org/docs/69483/narrative/).
Funding: Reported; funded by US VA/DoD.
Conflicts of Interested: Reported; detained in Section VI-C. One surgeon removed from panels after CoI adjudicated.
Key References:
- Galliker G, Scherer DE, Trippolini MA, Rasmussen-Barr E, LoMartire R, Wertli MM. Low back pain in the emergency department: Prevalence of serious spinal pathologies and diagnostic accuracy of red flags. Am J Med. 2020;133(1):60-72.e14. Epub 2019/07/07. doi: 10.1016/j.amjmed.2019.06.005. PubMed PMID: 31278933.
- Upadhye S, Kumbhare D. What Are the Most Useful Red Flags for Suspected Vertebral Fracture in Patients with Low Back Pain in the Emergency Department? Annals Emerg Med 2016; 67(1): 81-82.
CPG Quality/ Trustworthiness Standards
Amalgamated from AGREE-II/NEATS instruments.
| Quality/Trustworthiness Domain | |
| The clinical practice guideline (CPG) discloses and states explicitly its funding source. | ✔ |
| Financial conflicts of interest of guideline development group (GDG) members have been disclosed and managed. Section VI-C | ✔ |
| The CPG development group includes all of the relevant multidisciplinary stakeholders, including clinicians, methodologists and patients/caregivers. Table 3 | ✔ |
| The CPG objectives, health questions, scope of relevant providers and target recipients of care are clearly defined. Appendix A | ✔ |
| Values/preferences of patients, caregivers, advocates and/or the public with experience with the clinical disease management has been sought/integrated into CPG development (reported clearly). Section VI-D, Appendix B | ✔ |
| The search strategy for evidence is thoroughly developed and described. Table A-3, Appendix H. | ✔ |
| The criteria for selecting relevant studies/evidence are clearly described. | ✔ |
| The quality, strengths and limitations of the body of evidence are clearly described (e.g., GRADE, Cochrane, etc.). Summaries of evidence tables are provided. Section VI-A, USPSTF methods handbook | ✔ |
| The health benefits, side effects, and risks were considered in formulating the recommendations. | ✔ |
| There is an explicit approach linking the evidence to formulate the recommendations. GRADE Evidence to Recs Framework; Table A-4 | ✔ |
| The strength of recommendations is clearly reported, including confidence in underlying evidence. | ✔ |
| Recommendations are clear and unambiguous, and easily identified in the CPG publication. Appendix C – Evidence Table | ✔ |
| Different options for management for managing the health questions are clearly presented. | ✔ |
| Experts externally reviewed the guideline prior to its publication. Section VI-E | ✔ |
| The CPG describes a procedure to update the guideline, and provides advice, tools and/or clinical pathways for easy adoption/adaptation into practice. Section VIII Algorithm | ✔ |
| The CPG describes barriers and facilitators to implement recommendations. Some reported | ? |
| Performance metrics for monitoring implementation of recommendations for audit/feedback have been defined appropriately. None listed; consider “Strong” Recs? | X |
| Resource implications for implementing CPG recommendations have been discussed. | ✔ |
ECRI Trust Score Card
