MONTHLY FEATURE CPG SOPR SUMMARY
CPG Citation: Silvers SM, Gemme SR, Hickey S, Mattu A, Jaukoos JS, Diercks DB, Wolf SJ. Clinical Policy: Critical Issues in the Evaluation and Management of Adult Patients Presenting to the Emergency Department With Acute Heart Failure Syndromes. Annals Emerg Med. 2022 Oct;80(4):e31-e59. doi: 10.1016/j.annemergmed.2022.05.027. PMID: 36153055
Downloadable at: https://www.acep.org/patient-care/clinical-policies/acute-heart-failure-syndromes/
Scope of Guideline: Guidance intended for all ED physicians/providers who manage acute heart failure syndrome (AHFS) patients.
Inclusion: Adult patients presenting to ED with AHFS. Definition of AHFS = “gradual or rapid deterioration in heart failure signs and symptoms resulting in a need for urgent therapy.” Deemed interchangeable with “acute (decompensated) heart failure.”
Exclusion: Patients with acute STEMI, high-output heart failure, cardiogenic shock, renal failure, valvular emergencies, pregnant adults and pediatric patients.

Summary download – click![]()
Key Words: Acute heart failure, diuretics, emergency department, point-of-care ultrasound (POCUS), risk-stratification tools, vasodilators.
Key Recommendations: Each recommendation is accompanied by the “strength” of recommendation and the level of evidence (LoE) supporting that recommendation
| Question | Recommendation (Strength) |
| Q1. In adult patients presenting to the ED with suspected AHFS, is the diagnostic accuracy of point-of-care lung ultrasound sufficient to direct clinical management? | Use point-of-care lung ultrasound (POCLUS) as an imaging modality in conjunction with medical history and physical examination to diagnose AHFS when diagnostic uncertainty exists, as the accuracy of this diagnostic test is sufficient to direct clinical management. (Level B; no Level A or C Rec). |
| Q2. In ED adult patients with suspected AHFS, is early administration of diuretics safe and effective? No Level A or B Recs. | Although no specific timing of diuretic therapy can be recommended, physicians may consider earlier administration of diuretics when indicated for ED AHFS patients, because it may be associated with reduced length of stay and in-hospital mortality (Level C; consensus). Physicians should be confident in the Dx of AHFS with volume overload in a patient before the administration of diuretics, as Rx with diuretics may cause harm to those with an alternative diagnosis (Level C; consensus). |
| Q3. In adult ED AHFS patients, is vasodilator therapy with high-dose nitroglycerin administration safe and effective? | Consider using high-dose nitroglycerin as a safe and effective treatment option when administered to patients with acute heart failure syndrome and elevated blood pressure (Level C; consensus). |
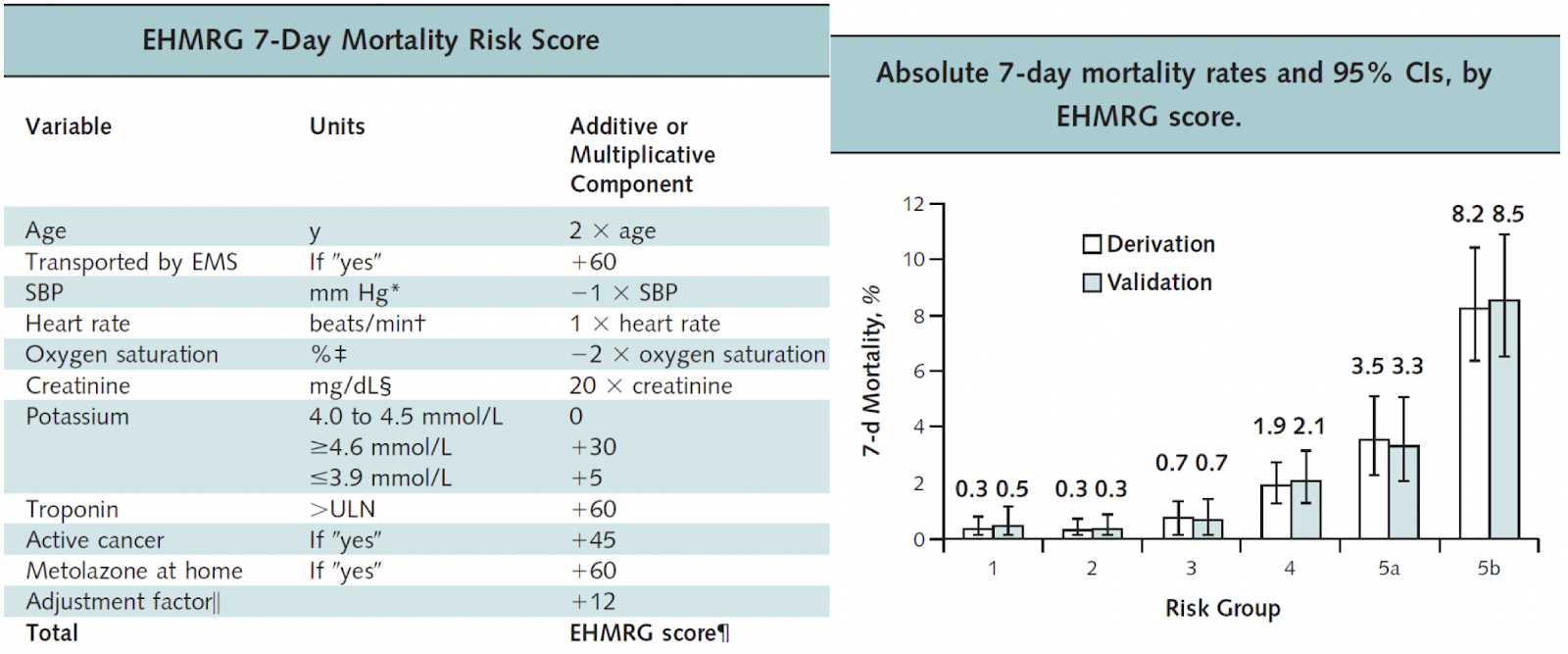
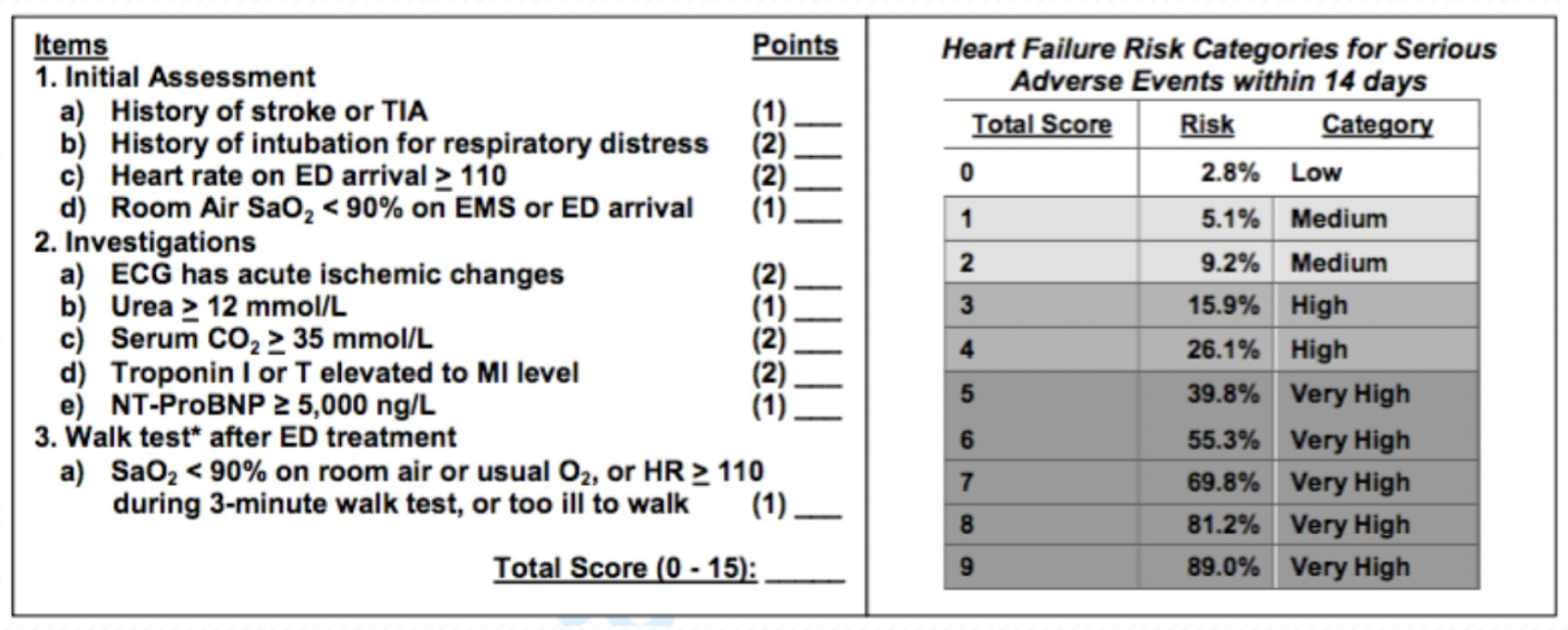
| Q4. In adult ED AHFS patients, is there a defined group that may be safely discharged home for outpatient follow-up? | Do not rely on current AHFS risk stratification tools alone todetermine which patients may be discharged directly homefrom the emergency department. Consider using the Ottawa Heart Failure Risk Scale (OHFRS) to help determine which higher-risk patients for adverse outcome should not be discharged home (Level B). Consider using the Emergency Heart Failure Mortality Risk Grade for 7-day mortality (EHMRG7) or the STRATIFY decision tool to help determine which higher-risk patients for adverseoutcome should not be discharged home (Level C). Use shared decision-making strategies when determining the appropriate disposition of AHFS patients (Consensus Rec). |
CLINICAL COMMENTARY:
- Acute heart failure continues to rise in North America, and is associated with 12% in-hospital mortality. Case fatality rates after initial AHF Dx remains at 10% at 30d, 22% at 1yr, and 42% at 5yrs. The health costs burden is expected to reach $USD70 billion by 2030. 80% of in-hospital cases are admitted via the ED.
- Accuracy of POCLUS by ED physicians will be dependent on operator training and experience (Q1). Recent literature confirms that ED physician diagnostic accuracy matches that of formal radiologists when properly applied. POCLUS is faster (<5min) and safer (non-ionizing) than traditional CXR, and has better Dx accuracy for pulmonary edema than either CXR or BNP labs. Incorporating POCLUS into a strategic Dx algorithm for AHFS improves Dx accuracy and accelerates acute management.
- Use of loop diuretics to reduce cardiac preload has been the mainstay of AHFS treatment for decades. Early Rx can decrease duration of symptoms, ED/hospital LOS and in-patient mortality. Clinicians should be confident that patients are fluid overloaded, however, in order to avoid inadvertent harms. The optimal timing of loop diuretics in the ED remains unclear.
- Use of nitroglycerin infusion may be reasonable in AHFS with high blood pressure (reduce preload and afterload). There may be benefits of reducing respiratory distress, need for intubation and ICU admissions. Higher doses, however, may increase risk of hypotension. NTG has rapid onset (3-5min, depending on delivery route), and a half-life of 2-7min. Optimal dosing, and timing of combined NTG with diuretics remains of uncertain.
- Using “validated” CDRs may be premature at this time, with the OHFRS tool having the “best” validation to date. However, there has not been a reliable cut-off score set for which patients can and cannot be safely discharged. The STRATIFY tool is still at the derivation level, and is quite difficult to use in ED settings. The EHMRG7 tool is also a bit complex for scoring, although online calculators are readily available (eg. MedCalc; see link below); this tool has been successfully used in a AHFS implementation trial recently published (Lee et al, NEJM 2022). Overall, use of these tools may benefit the patient by reducing the risk of short-term adverse events after ED discharge. However, using these tools could increase hospital admissions, which may lead to different complications and over-crowding concerns. It may be most prudent to use these tools in a shared decision-making discussion with patients re: potential ED discharge, accounting for other safe discharge concerns (eg. follow-up, home safety, ability to return to ED if worsening, etc.). The utility of search AHFS CDRs has been previously reviewed (Michaud et al, Can J Cardiol 2018).
Benefits, Harms & Adverse of Recommendations: All explicitly discussed with each PICOT Q and Rec. Summarized in Clinical Commentary points above.
Facilitators of Uptake: A structured approach (ie. clinical carepath/protocol) for ED AHFS, with built-in POCLUS and validated risk-stratification tools, can be used to rapidly diagnose, manage and disposition such patients. Such a structured pathway has been successfully implemented in a cluster RCT in Ontario, Canada (Lee el al, COACH trial NEJM 2022). Integrating various sources of trustworthy high-quality evidence into a novel ED pathway should optimize patient outcomes.
Barriers to Uptake: A summary of Recs should ideally be presented at the beginning of the document, as this is a preferred attribute for EM CPG consumers (Aboulsoud et al, Int J Emerg Med 2011). Also, there are no clinical algorithms/pathways for EM physicians to adopt/adapt to their workplaces (#1 preferred EM CPG attribute). Clinical training and experience in POCLUS may limit the applicability of this diagnostic modality at the bedside, although it seems to be equivalent/superior to CXR diagnosis.
Prior Guideline Recommendations/Relevant Evidence: This Policy updates prior guidance from ACEP 2007.
Disclaimer (if any stated): Policy is NOT meant to define standard of care for ED AHFS. “ACEP recognizes the importance of the individual physician’s judgment and patient preferences. This guideline provides clinical strategies for which medical literature exists to inform the critical questions addressed in this policy.”
Funding: (Reported): ACEP Clinical Policies committee.
Conflicts of Interested: (Reported) No conflicts of interest to declare.
Supporting Literature:
- Lee DS, Straus SE, Farkouh ME, et al; COACH Trial Investigators. Trial of an Intervention to Improve Acute Heart Failure Outcomes. N Engl J Med. 2022 Nov 5.
doi: 10.1056/NEJMoa2211680 PMID: 36342109
- Aboulsoud S, Huckson S, Wyer P, Lang E. Survey of preferred guideline attributes: what helps to make guidelines more useful to emergency health practitioners. Int J Emerg Med 2012; 5:42-29. DOI: 10.1186/1865-1380-5-42 PMID: 23140222
- Michaud AM, Parker SIA, Ganshorn H et al. Prediction of Early Adverse Events in Emergency Department Patients With Acute Heart Failure: A Systematic Review. Can J Cardiol 2018; Vol 34(2): 168-179. DOI:https://doi.org/10.1016/j.cjca.2017.09.004
CPG Quality/ Trustworthiness Standards
Amalgamated from AGREE-II/NEATS instruments.
| The clinical practice guideline (CPG) discloses and states explicitly its funding source. ACEP | ✔ |
| Financial conflicts of interest of guideline development group (GDG) members have been disclosed and managed. No relevant conflicts reported. | ✔ |
| The CPG development group includes all of the relevant multidisciplinary stakeholders, including clinicians, methodologists and patients/caregivers. Group included resident reps, and patient safety advocates. No actual patients/caregivers reported. | ? |
| The CPG objectives, health questions, scope of relevant providers and target recipients of care are clearly defined. | ✔ |
| Values/preferences of patients, caregivers, advocates and/or the public with experience with the clinical disease management has been sought/integrated into CPG development (reported clearly). | X |
| The search strategy for evidence is thoroughly developed and described. 2 librarians, limited to English language articles. | ✔ |
| The criteria for selecting relevant studies/evidence are clearly described. | ✔ |
| The quality, strengths and limitations of the body of evidence are clearly described (e.g., GRADE, Cochrane, etc.). Summaries of evidence tables are provided. Usual ACEP Policy frameworks. | ✔ |
| The health benefits, side effects, and risks were considered in formulating the recommendations. Potential benefits & harms reviewed with each Rec. | ✔ |
| There is an explicit approach linking the evidence to formulate the recommendations. Level A/B/C | ✔ |
| The strength of recommendations is clearly reported, including confidence in underlying evidence. | ✔ |
| Recommendations are clear and unambiguous, and easily identified in the CPG publication. | ✔ |
| Different options for management for managing the health questions are clearly presented. | ✔ |
| Experts externally reviewed the guideline prior to its publication. External review by ACEP community, other EM organizations. | ✔ |
| The CPG describes a procedure to update the guideline. Goal to update every 3yrs. | ✔ |
| The CPG provides advice, tools and/or clinical pathways for easy adoption/adaptation into practice. | X |
| The CPG describes barriers and facilitators to implement recommendations. | X |
| Performance metrics for monitoring implementation of recommendations for audit/feedback have been defined appropriately. | X |
| Resource implications for implementing CPG recommendations have been discussed. | ✔ |
Methodological threats to validity:
- As with many ACEP Policies, there is a lack of patient/caregiver/public stakeholder engagement which can lead to PICOT questions and Recs that are not necessarily patient-centred.
- ACEP evaluation of evidence uses the original 1993 Rec A/B/C & Evidence I/II/III rating framework, which is not necessarily intuitive for readers, and inconsistent with most international guideline organizations that have embrace GRADE methodologies.
- All Recs are either Level B or C, reflecting the relative paucity/weakness of the evidence supporting them. These should NOT, therefore, necessarily be used in creating quality improvement performance metrics (which should be ideally limited to Strong/Level A Recs based on high certainty/quality of supporting evidence).
- ACEP strives to update their Policies every 3-5 years, but this one is 15yrs after the original 2007 document.
Ottawa Heart Failure Risk Score (OHFRS): Available online at https://www.mdcalc.com/calc/3994/ottawa-heart-failure-risk-scale-ohfrs
EHMRG7 Score: available online at https://www.mdcalc.com/calc/1755/emergency-heart-failure-mortality-risk-grade-ehmrg.