MONTHLY FEATURE CPG SOPR SUMMARY
CPG Citation: American Academy of Orthopaedic Surgeons Management of Hip Fractures in Older Adults Evidence-Based Clinical Practice Guideline. https://www.aaos.org/hipfxcpg. Published 12/03/2021
Scope of Guideline: Adults >55yo with hip fracture.
Inclusion: Adults with acute hip perioperative hip fracture.
Exclusion: Prevention of primary/secondary hip fractures, post-hospital rehabilitation.
Key Words: Hip fracture, analgesia, traction, transfusion, TXA.
Summary download – click![]()
Key Recommendations: Each recommendation is accompanied by the “strength” of recommendation and the level of evidence (LoE) supporting that recommendation
| Recommendations | Strength (LoE) |
| FOR Clinical Action | |
| Venous thromboembolism (VTE) prophylaxis should be used in hip fracture patients. | Strong (Moderate) |
| Multimodal analgesia incorporating preoperative nerve block is recommended to treat pain after hip fracture. | Strong (Strong) |
| Tranexamic acid should be administered to reduce blood loss and blood transfusion in patients with hip fractures. | Strong (Strong) |
| NEUTRAL Clinical Action | |
| A blood transfusion threshold of no higher than 8g/dl is suggested inasymptomatic postoperative hip fracture patients. | Moderate (Moderate) |
| AGAINST Clinical Action | |
| Preoperative traction should not routinely be used for patients with a hip fracture. | Strong (Strong) |
Benefits vs. Harms/Adverse Effects of Recommendations:
The Recs most likely relevant to EM practice is the prohibition of preoperative traction, TXA/ transfusions for significant blood loss, and the use of multimodal analgesia incorporating preoperative nerve block for pain control.
For patients with significant blood loss in trauma (including hip fracture), the use of TXA is “Strongly” recommended, and this is congruent with other contemporary trauma/transfusion guidelines. A transfusion of threshold of 8g/dl is reasonable, and likely congruent with other trauma transfusion guidelines. If the patient will be in the ED for an extended period of time awaiting operative repair, then initiating VTE prophylaxis (VTEP) is appropriate; ideally your Orthopedic colleagues will have created a hip fracture care pathway that will incorporate VTEP that could be initated in the ED.
There is an abundance of high-quality reviews supporting the use of peripheral nerve blockade over many years/trials, and could be considered standard of care in ED hip fracture analgesia. This is a skill that should be taught to trainees as part of their POCUS curriculum, and practicing staff physicians could easily be trained in this relatively easy procedure. The patient benefits include rapid onset of effective analgesia, reduced levels of delirium and opioid sparing. Harms may include a missed block, accidental injury to femoral vessels and surrounding tissues, puncture wound infections, and nerve injury if directly injected. Most of these, however, can be obviated by using a slow and careful procedure technique with US guidance. Finally, an accidental intravenous injection of anesthetics can lead to toxicity reactions, so having IntraLipid antidote on hand is also wise.
Barriers to Uptake: The most significant barrier to using nerve blocks will likely be training, experience and availability of US for proper guidance. Lack of appropriate equipment (sterile?) may also be a challenge in providing timely blocks in the ED.
VTEP without an institutional care path may be an uncertain undertaking for ED physicians who may not be aware of latest VTEP guidance.
Facilitators of Uptake: Formal training courses are readily available for use of US-guided injection procedures in the ED, and a plethora of training videos are also accessible online. The NYSORA website has many educational videos for US guided procedures relevant to ED practice (https://www.youtube.com/watch?v=tMy978ZwaDU). This is an intervention that is ideally suited for an ED Quality Improvement/Patient Safety (QIPS) program, as the performance metrics for such are easily measured and improvable.
A dedicated nerve block kit/equipment box is also ideal to ensure access to all required equipment, but the individual components are also readily available throughout most ED procedure rooms/carts.
VTEP guidance should be operationalized by Orthopedic, Thrombosis and other relevant services into a hip fracture care path to optimize and standardize care of such patients, including preliminary orders that can be initiated in the ED setting.
Key References:
- Guay J, Kopp S. Peripheral nerve blocks for hip fractures in adults.
Cochrane Database of Systematic Reviews 2020, Issue 11. Art. No.: CD001159.
DOI: 10.1002/14651858.CD001159.pub3.
- Ritcey B, Pageau P, Woo MY, Perry JJ. Regional Nerve Blocks for Hip and Femoral Neck Fractures in the Emergency Department: A Systematic Review. Can J Emerg Med 2016; 18(1): 37-47. DOI 10.1017/cem.2015.75
- Nagdev A, Mantuani N. Avoid These Two Common Femoral Nerve-Block Errors. ACEP Now (2019) https://www.acepnow.com/article/avoid-these-two-common-femoral-nerve-block-errors/
- Morgenstern J. Femoral Nerve Blocks – The Evidence. First10EM (2018) https://first10em.com/femoral-nerve-blocks/
- Vermeulen M, Otterness K. Practical Tips: How and When to Use a Femoral Nerve Block. EM Resident (2014) https://www.emra.org/emresident/article/practical-tips-when-and-how-to-use-a-femoral-nerve-block/
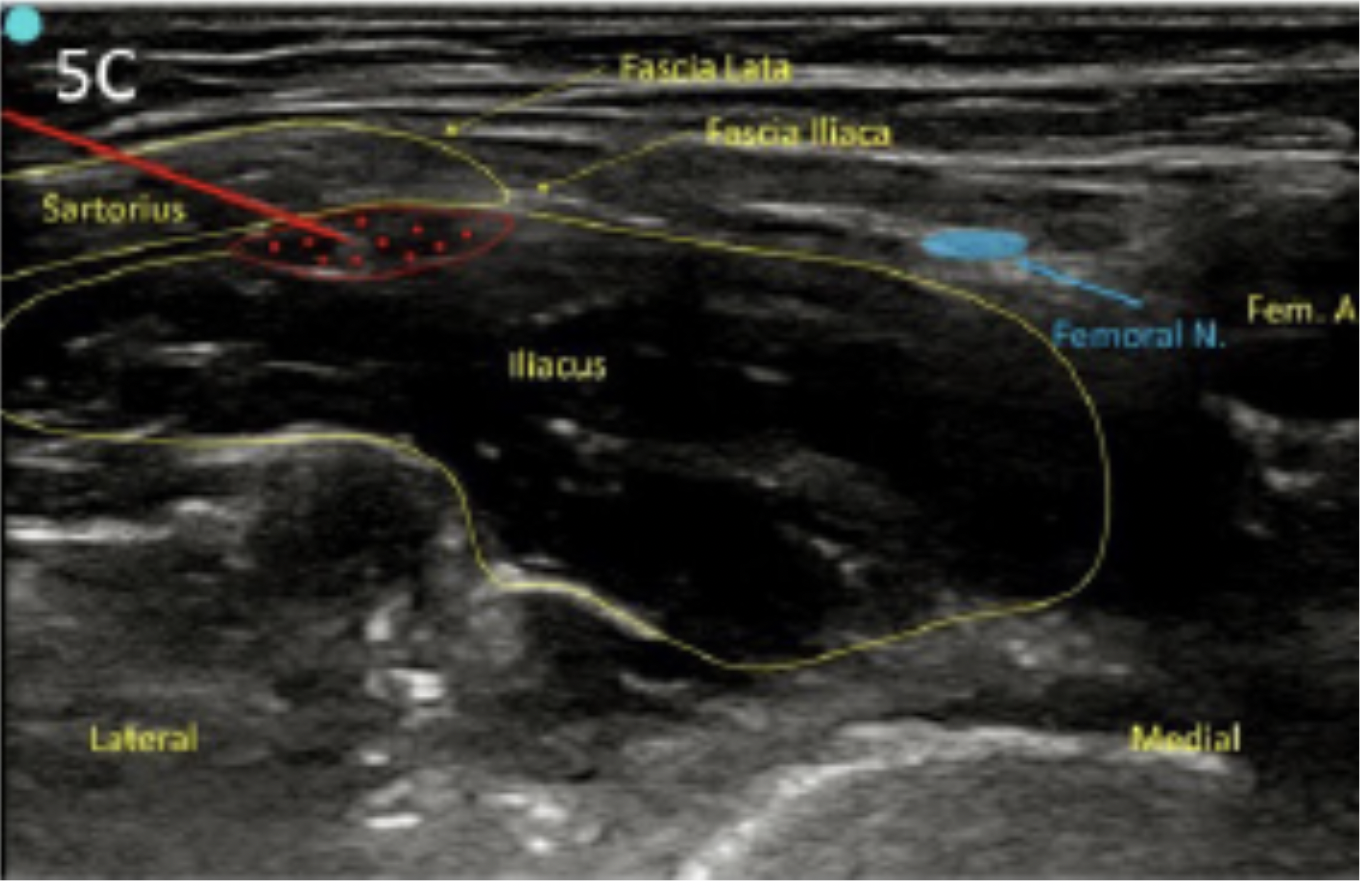
Relevant US Imaging for Femoral Nerve Block for ED Hip Fracture
CPG Quality/ Trustworthiness Standards
Amalgamated from AGREE-II/NEATS instruments.
| Quality/Trustworthiness Domain | |
| The clinical practice guideline (CPG) discloses and states explicitly its funding source. | ✔ |
| Financial conflicts of interest of guideline development group (GDG) members have been disclosed and managed. | ✔ |
| The CPG development group includes all of the relevant multidisciplinary stakeholders, including clinicians, methodologists and patients/caregivers. ER physician on development panel; no patient/caregiver perspectives reported. | ? |
| The CPG objectives, health questions, scope of relevant providers and target recipients of care are clearly defined. | ✔ |
| Values/preferences of patients, caregivers, advocates and/or the public with experience with the clinical disease management has been sought/integrated into CPG development (reported clearly). No specific patient values/preferences for outcomes reported. | X |
| The search strategy for evidence is thoroughly developed and described. E-Appendix1? | ? |
| The criteria for selecting relevant studies/evidence are clearly described. Appendix II | ✔ |
| The quality, strengths and limitations of the body of evidence are clearly described (e.g., GRADE, Cochrane, etc.). Summaries of evidence tables are provided. GRADE used; no summary tables provided. | ✔ |
| The health benefits, side effects, and risks were considered in formulating the recommendations. | ✔ |
| There is an explicit approach linking the evidence to formulate the recommendations. | ✔ |
| The strength of recommendations is clearly reported, including confidence in underlying evidence. | ✔ |
| Recommendations are clear and unambiguous, and easily identified in the CPG publication. | ✔ |
| Different options for management for managing the health questions are clearly presented. | ✔ |
| Experts externally reviewed the guideline prior to its publication. | ✔ |
| The CPG describes a procedure to update the guideline, and provides advice, tools and/or clinical pathways for easy adoption/adaptation into practice. | ✔ |
| The CPG describes barriers and facilitators to implement recommendations. | ✔ |
| Performance metrics for monitoring implementation of recommendations for audit/feedback have been defined appropriately. Not specifically stated, but Strong Recs above are easily measured with administrative data (except use of hip traction?). | ? |
| Resource implications for implementing CPG recommendations have been discussed. Deliberately excluded. | X |
Guideline Key Features
- Funding: Reported; funding by AAOS; no external funding.
- Conflicts of Interest: Reported; no significant conflicts reported . Reported in Appendix III.
- Panelists: Included one Emergency Physician (ACEP representative).