MONTHLY FEATURE CPG SOPR SUMMARY
CPG Citation: Katz PO, Dunbar KB, Schnoll-Sussman FH, Greer KB, Yadlapati R, Spechler SJ. ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease. Am J Gastroenterol 2022; 117(1):27-56. PMID: 34807007
Downloadable at: DOI: 10.14309/ajg.0000000000001538
Scope of Guideline: Clinicians caring for GERD patients.
Inclusion: Not specified. Exclusion: Not specified.
Key Words: GERD, heartburn, chest pain, proton-pump inhibitors.

Summary download – click![]()
Key Recommendations: Each recommendation is accompanied by the “strength” of
recommendation and the level of evidence (LoE) supporting that recommendation.
Only Recs relevant to EM practice are listed (not outpatient/specialist clinics).
| Recommendations | Strength, LoE |
| FOR Clinical Action For patients with classic GERD symptoms of heartburn and regurgitation who have no alarm symptoms, we recommend an 8-wk trial of empiric PPIs once daily before a meal. | Strong (Mod) |
| We recommend endoscopy as the first test for evaluation of patients presenting with dysphagia or other alarm symptoms (weight loss and GI bleeding) and for patients with multiple risk factors for Barrett’s esophagus. | Strong (Low) |
| We recommend weight loss in overweight and obese patients for improvement of GERD symptoms. | Strong (Mod) |
| We recommend treatment with PPIs over treatment with H2RA for healing erosive esophagitis (EE). | Strong (High) |
| We recommend treatment with PPIs over H2RA for maintenance of healing for EE. | Strong (Mod) |
| We recommend PPI administration 30–60 min before a meal rather than at bedtime for GERD symptom control. | Strong (Mod) |
| We recommend evaluation for non-GERD causes in patients with possible extraesophageal manifestations before ascribing symptoms to GERD. | Strong (Mod) |
| We recommend evaluation for non-GERD causes in patients with possible extraesophageal manifestations before ascribing symptoms to GERD. | Strong (Mod) |
| We recommend optimization of PPI therapy as the first step in management of refractory GERD. | Strong (Mod) |
| NEUTRAL Clinical Action In patients with chest pain who have had adequate evaluation to exclude heart disease, objective testing for GERD (endoscopy and/or reflux monitoring) is recommended. | Conditional (Low) |
| We recommend that patients who have extraesophageal manifestations of GERD without typical GERD symptoms (e.g., heartburn and regurgitation) undergo reflux testing for evaluation before PPI therapy. | Strong (Mod) |
| AGAINST Clinical Action We do not recommend baclofen in the absence of objective evidence of GERD.We recommend against treatment with a prokinetic agent of any kind for GERD therapy unless there is objective evidence of gastroparesis. | Strong (Mod) Strong (Low) |
| We do not recommend sucralfate for GERD therapy except during pregnancy. | Strong (Low) |
Benefits of Recommendations: A number of Strong Recs are offered here that may have
utility in ED practice (most with Moderate supporting evidence). It is most important to rule out dangerous diagnoses with abdominal/chest pain in the ED, and GERD will likely be a diagnosis of exclusion/history.
It may be reasonable to initiate a trial of PPI’s in the ED (short course 4-8 weeks) with an appropriate follow-up (or out-patient referral) with other physicians/specialists as available in your ED. Use of sulcrate may be appropriate to consider in pregnant patients (unabsorbed, minimal systemic toxicity).
HarmsAdverse Effects of Recommendations: Certain medications have side effects that are not reasonable to embrace in the ED setting (prokinetics [metoclopramide], baclofen). All histamine H2-blockers are FDA category B, and all PPIs are FDA category B (except omeprazole), which is FDA category C.
Barriers to Uptake: None noted.
Facilitators of Uptake: None noted.
CLINICAL COMMENTARY:
GERD definitions used in this CPG (blended from prior literature): GERD is the condition in which the reflux of gastric contents into the esophagus results in symptoms and/or complications. GERD is objectively defined by the presence of characteristic mucosal injury seen at endoscopy and/or abnormal esophageal acid exposure demonstrated on a reflux monitoring study. A response to PPI’s is NOT considered a reliable confirmation of GERD diagnosis (Sens 78%, Spec 54%).
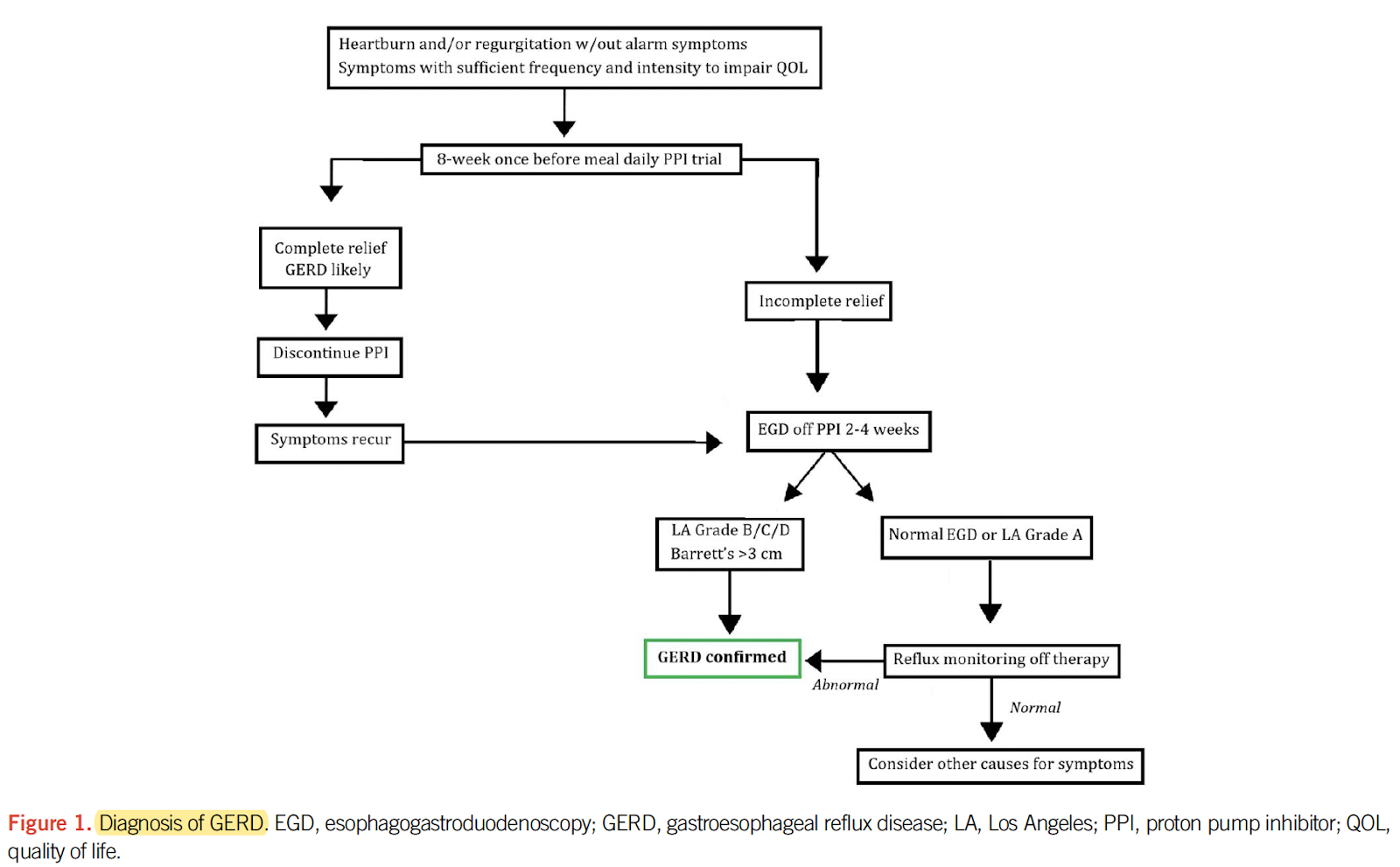
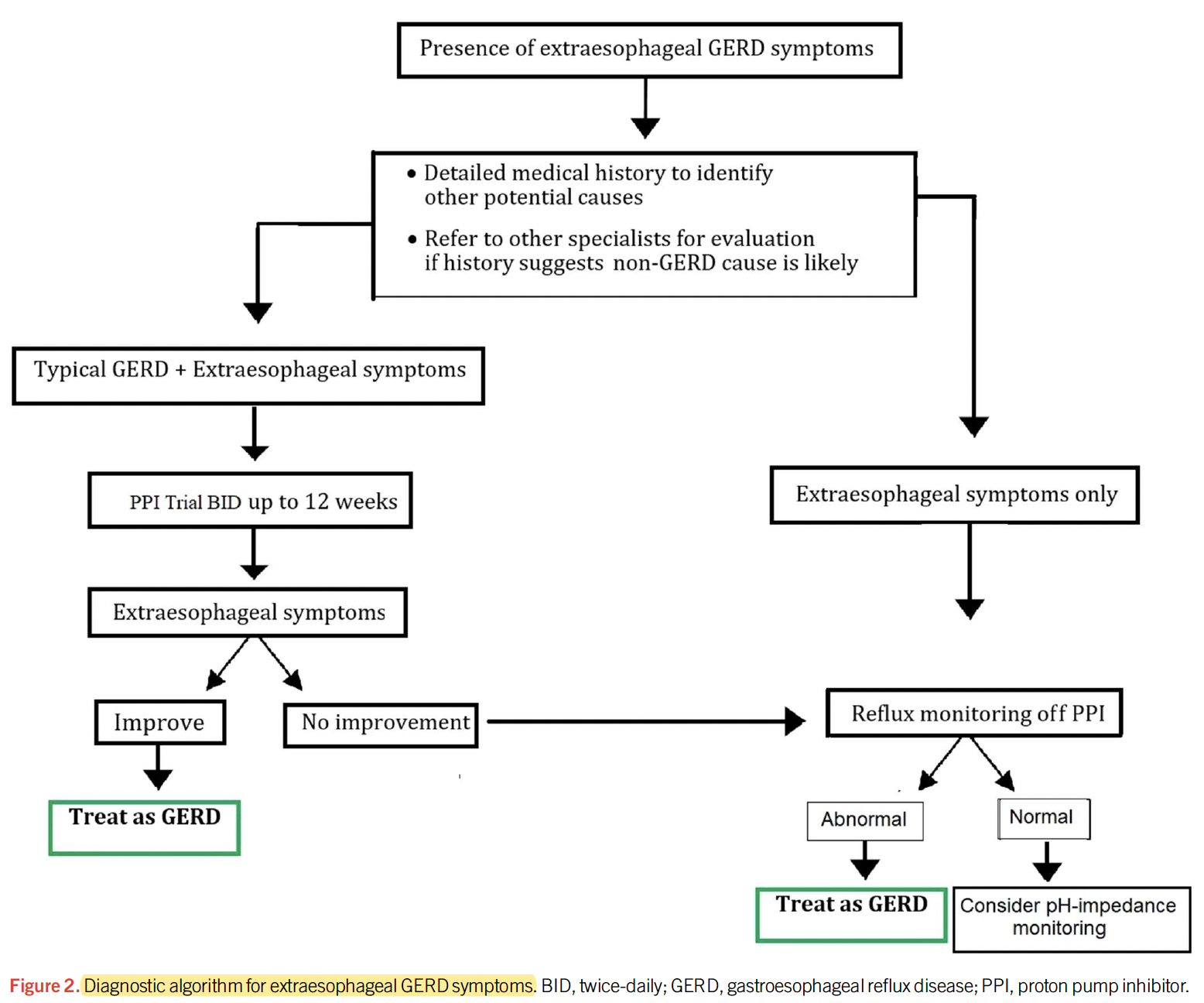
The most common symptoms (Sens 33-76%, Spec 62-96%) of GERD include heartburn symptoms in the chest, and regurgitation (with bitter/acid taste in mouth). Symptoms may be nonspecific, however, and overlap with other GI conditions (hiatus hernia, achalasia, eosinophilic esophagitis, reflux hypersensitivity) and cardiac or respiratory symptoms (hoarseness, throat clearing, chronic cough, laryngitis, pharyngitis, pulmonary fibrosis/ progressive dyspnea). Presence of extra-esophageal symptoms are neither inclusive or exclusive of GERD; these conditions should be ruled out in ED as warranted. A diagnostic algorithm for GERD is presented in Figure 1 below. Common extra-esophageal symptoms (chronic cough, throat-clearing, hoarseness, globus sensation, laryngitis, asthma) merit appropriate investigations by specialists once dangerous conditions in the ED are excluded. An approach to extra-esophageal symptoms is shown in Figure 2.
Weak lifestyle recommendations that may be helpful in GERD management control include avoiding meals/snacks 2-3hrs before bedtime, avoiding “trigger” foods (>6 cups of coffee/carbonated drinks, chocolate, spicy/acidic/high fat content foods), smoking reduction/cessation, and sleeping with head elevated 30degrees (all Conditional Recs, low LoE). Limited evidence also suggest reducing alcohol consumption. There may also be a benefit in sleeping left-side down, as the right-side down position puts the EG junction in a dependent position relative to pooled gastric contents that favours reflux action.
With a presumptive Dx of GERD in the ED (assuming all other important diagnoses excluded), it is most appropriate to start medical Rx with PPI’s (over H2-blockers, sulcrate, promotility agents, baclofen). There is little likely difference in which PPI’s are most beneficial for GERD healing/long-term symptom control. They should best be taken before meals (since meals are the key acid-secreting trigger), and are less effective at bedtime (no meal triggers). Alginate antacids may be useful for acute symptom control, but have no effect on erosive healing. Use of night-time H2-blockers may be helpful for nocturnal symptoms (with evidence of nocturnal GERD on pH testing despite PPI use).
GERD in pregnancy (66% incidence) increases in any trimester, even in those mothers with no GERD history, and usually resolves after delivery. Significant weight gain may be a predictor for persistent GERD 1yr post-delivery. Use of typical GERD medications may be limited in pregnant patients (eg. sulcrate only).
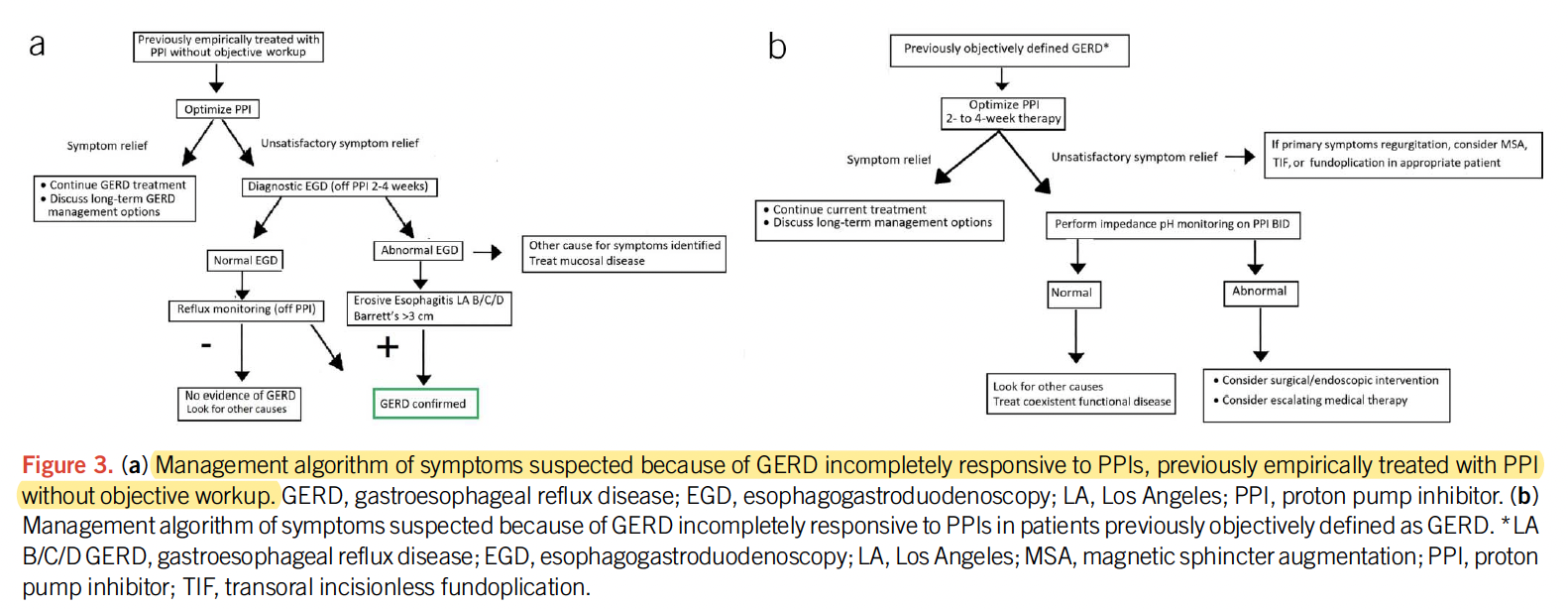
Patients with unconfirmed/refractory GERD and repeat ED visits may warrant an outpatient GI/surgery referral for further investigations (eg. endoscopy, biopsy, manometry, reflux monitoring) and optimization of care (including surgery). For patients with GERD symptoms who also have alarm symptoms (dysphagia, weight loss, GI bleeding, vomiting, and/or anemia), referral for endoscopy should be performed as soon as feasible. Figure 3 below outlines a diagnostic approach for PPI-refractory GERD.
Prior Guideline Recommendations/Relevant Evidence: This is an update of a prior 2013 publication.
Funding: Reported; none
Conflicts of Interested: Reported; numerous financial/industry CoI’s reported
CPG Quality/ Trustworthiness Standards
Amalgamated from AGREE-II/NEATS instruments.
| Quality/Trustworthiness Domain | |
| The clinical practice guideline (CPG) discloses and states explicitly its funding source. | ✔ |
| Financial conflicts of interest of guideline development group (GDG) members have been disclosed and managed. Conflicts reported; how managed? | ? |
| The CPG development group includes all of the relevant multidisciplinary stakeholders, including clinicians, methodologists and patients/caregivers. No patients/caregivers. | X |
| The CPG objectives, health questions, scope of relevant providers and target recipients of care are clearly defined. | ? |
| Values/preferences of patients, caregivers, advocates and/or the public with experience with the clinical disease management has been sought/integrated into CPG development (reported clearly). No comments on seeking PVP directly or literature search. | X |
| The search strategy for evidence is thoroughly developed and described. See below. | ? |
| The criteria for selecting relevant studies/evidence are clearly described. See below. | ? |
| The quality, strengths and limitations of the body of evidence are clearly described (e.g., GRADE, Cochrane, etc.). Summaries of evidence tables are provided. See below. | ? |
| The health benefits, side effects, and risks were considered in formulating the recommendations. Little comment on harms and risks included. | X |
| There is an explicit approach linking the evidence to formulate the recommendations. GRADE | ✔ |
| The strength of recommendations is clearly reported, including confidence in underlying evidence. GRADE | ✔ |
| Recommendations are clear and unambiguous, and easily identified in the CPG publication. | ✔ |
| Different options for management for managing the health questions are clearly presented. | ✔ |
| Experts externally reviewed the guideline prior to its publication. None reported. | X |
| The CPG describes a procedure to update the guideline, and provides advice, tools and/or clinical pathways for easy adoption/adaptation into practice. Algorithms included. | ✔ |
| The CPG describes barriers and facilitators to implement recommendations. | X |
| Performance metrics for monitoring implementation of recommendations for audit/feedback have been defined appropriately. Various “Strong” Recs with high LoE amenable for use as PMs. | X |
| Resource implications for implementing CPG recommendations have been discussed. | X |
Authors claim to have formulated relevant PICOT questions to be addressed, completed literature searches with a medical librarian, evaluated retrieved literature and formulated recommendations using GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) methods, incorporating the quality of evidence, risks vs. benefits, feasibility, and costs/resources based on patient/population-based factors. NO DETAILS of any of these key Methods steps are reported, and are not available online as supplementary materials.