MONTHLY FEATURE CPG SOPR SUMMARY
CPG Citation: Qaseem A, Etxeandia-Ikobaltzeta I, Lin JS, Fitterman N, Shamliyan T, Wilt TJ for the Clinical Guidelines Committee of the American College of Physicians. Diagnosis and Management of Acute Left-Sided Colonic Diverticulitis: A Clinical Guideline From the American College of Physicians. Ann Intern Med. 2022;175:399-415. doi:10.7326/M21-2710.
Downloadable at: https://doi.org/10.7326/M21-2710
**Accompanying Systematic Review: Balk EM, Adam GP, Bhuma MR, et al. Diagnostic imaging and medical management of acute left-sided colonic diverticulitis. A systematic review. Ann Intern Med. 2022; 175: 379-387. doi:10.7326/M21-1645
Scope of Guideline: All clinicians who care for patients with acute colonic diverticulitis.
Inclusion: Patients with suspected or confirmed acute colonic diverticulitis.
Exclusion: Patients with right- or complicated left-sided diverticulitis, SIRS/sepsis, immunosuppression, unstable comorbidities, concurrent antibiotics usage, need immediate surgery, acute renal injury, other sinister colonic pathology.

Key Words: acute colonic diverticulitis, antibiotics, imaging, outpatient management.
Summary download – click![]()
Key Recommendations: Each recommendation is accompanied by the “strength” of recommendation and the level of evidence (LoE) supporting that recommendation
| Recommendations | Strength, LoE |
| FOR Clinical Action | |
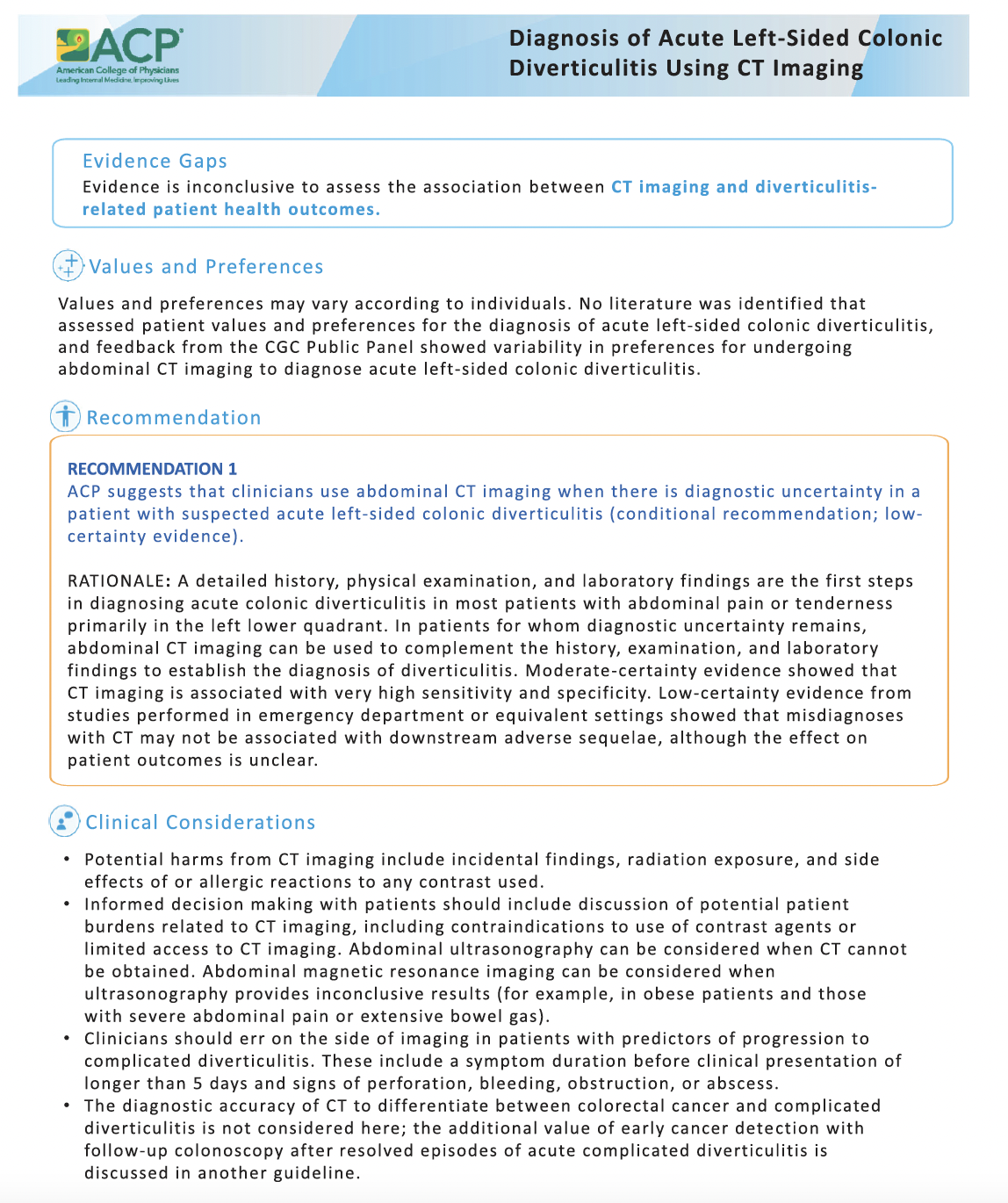
| Clinicians could use abdominal CT imaging when there is diagnostic uncertainty in a patient with suspected acute left-sided colonic diverticulitis. | Conditional, Low |
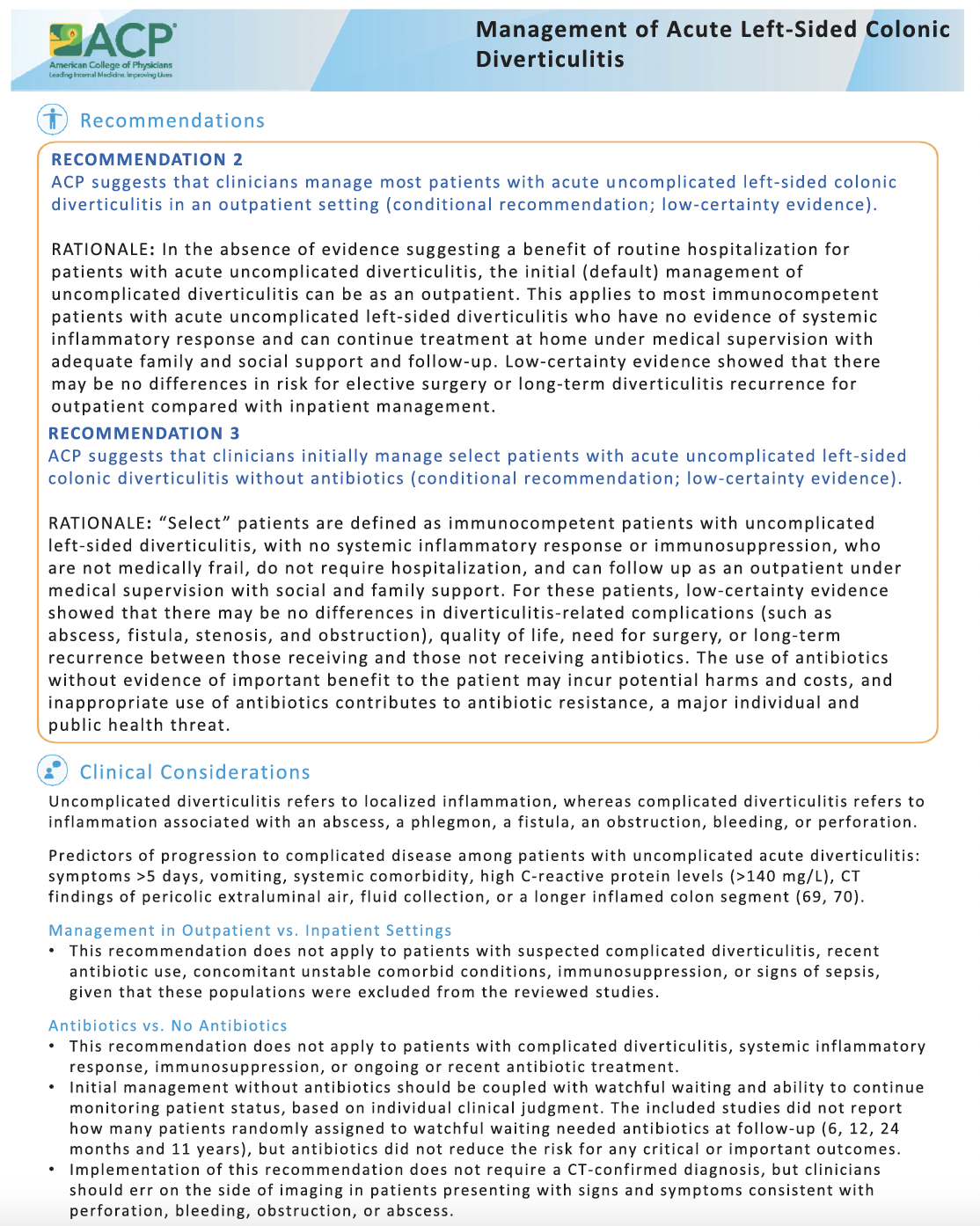
| Clinicians could manage most patients with acute uncomplicated left-sided colonic diverticulitis in an outpatient setting. | Conditional, Low |
| Clinicians initially could manage select patients with acute uncomplicated left-sided colonic diverticulitis without antibiotics. | Conditional, Low |
CLINICAL COMMENTARY:
About 5-10% of patients with diverticulosis will develop acute colonic diverticulitis (ACD), and risk increases with age. Prevalence of right-sided ACD is higher in Asian countries, whereas left-sided disease is more common in Western countries. About 12% of cases are complicated by inflammatory fistulae, abscess, phlegmon, obstruction, bleeding or perforations. The recurrence rates at 10yrs are about 22% after an initial event, and up to 55% after secondary attacks. The annual hospitalization costs for ACD have reached upwards of $USD8billion in recent years.
Many ED patients with abdominal pain (acute, recurrent) receive invasive investigations, and repeat CT scans which can result in long-term harms. Updates on managing low-risk recurrent abdominal pain have been recently reviewed in the Society for Academic Medicine GRACE-2 (Guidelines for Reasonable & Appropriate Care in Emergency room) publication (May 2022; downloadable at https://onlinelibrary.wiley.com/doi/10.1111/acem.14495) [DISCLOSURE: S. Upadhye is an author on GRACE-2 guidelines].
Benefits of Recommendations: Given the low certainty of evidence supporting CPG questions, ED physicians could consider following the stated Recs, but there is not higher supporting evidence guiding physicians as to what they should do…
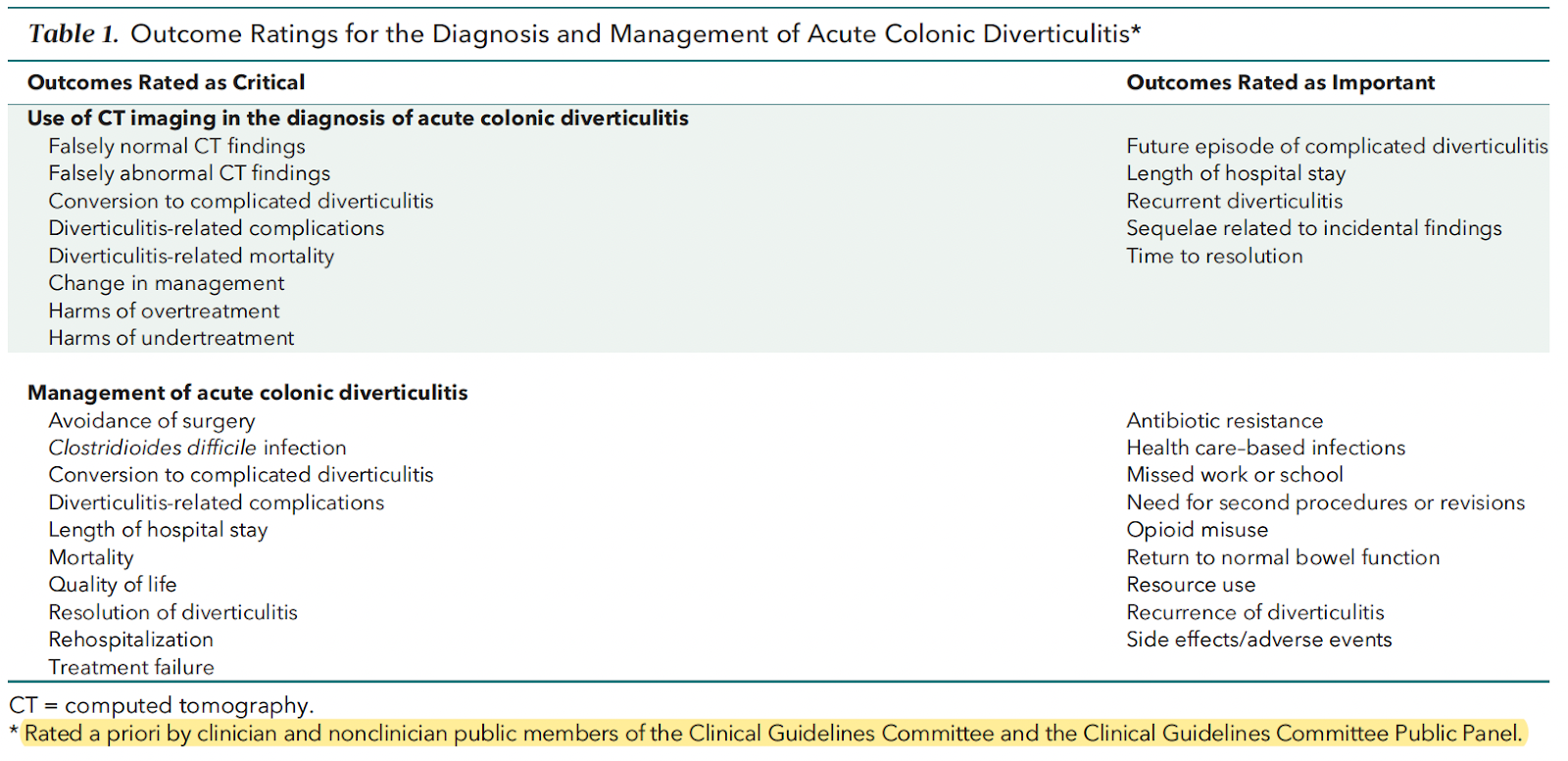
This CPG made a deliberate effort to solicit and rank Patient-Relevant Outcomes (PROs) amongst panelists (including public/patient stakeholders); these are summarized in Table 1.
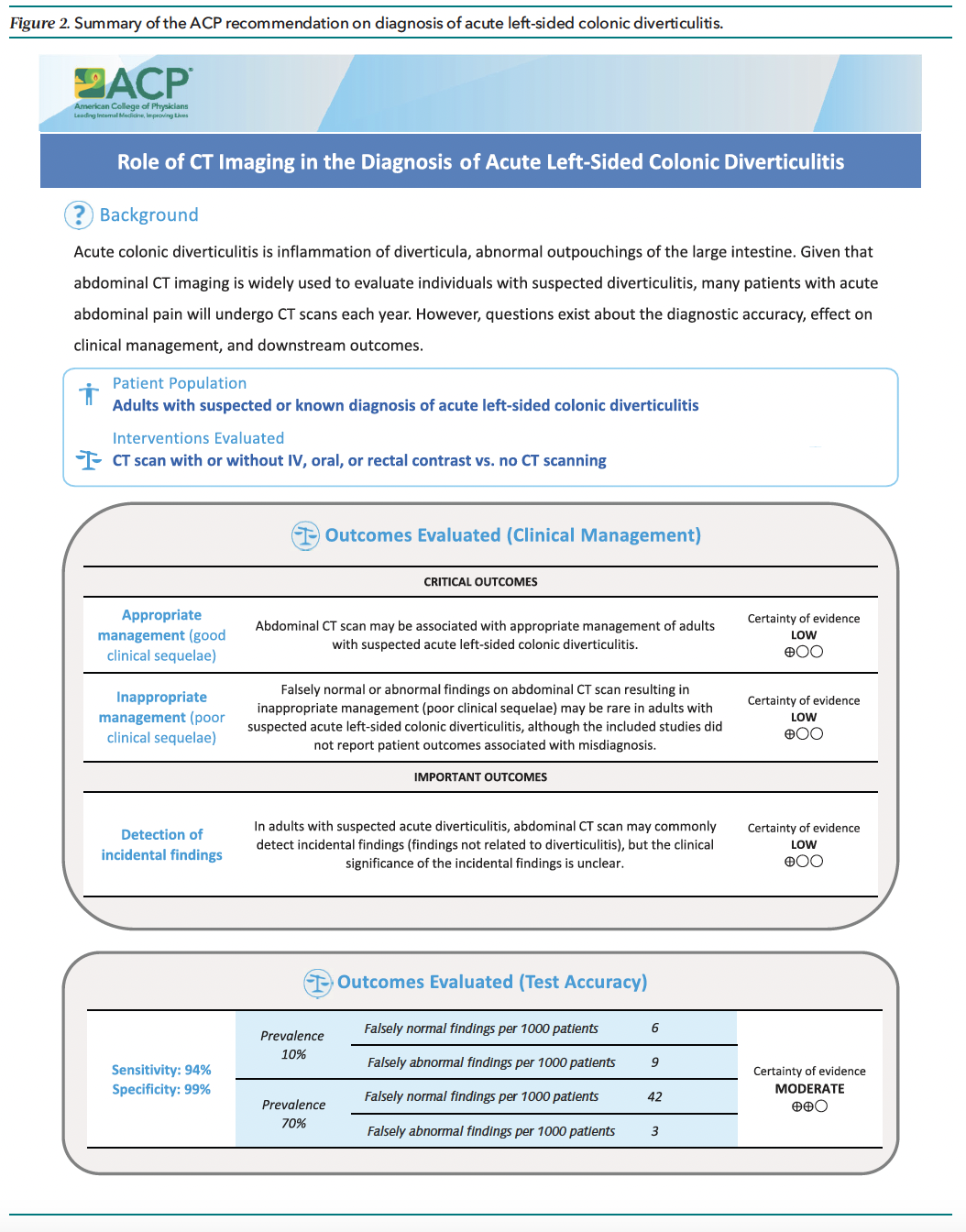
The diagnostic accuracy of contrast CT for acute left-sided diverticulitis from pooled studies was Sens 94% (95%CI 87-97%), and Spec 99% (90-99%), which is corresponds to a LR+ 94 and LR- 0.06, confirming that this is a very useful diagnostic discriminatory test. Based on a prevalence range from 10-70%, 6-42 per 1000 patients would have false negative results, and 3-9 per 1000 patients would have a false abnormal finding. These are summarized in Figure 2 below.
Managing low-risk patients in an outpatient setting was not unsafe compared to inpatient treatment (OR 0.85, 0.5-1.43), when considering outcomes of elective surgery or recurrence rates (low certainty evidence, 6 studies).
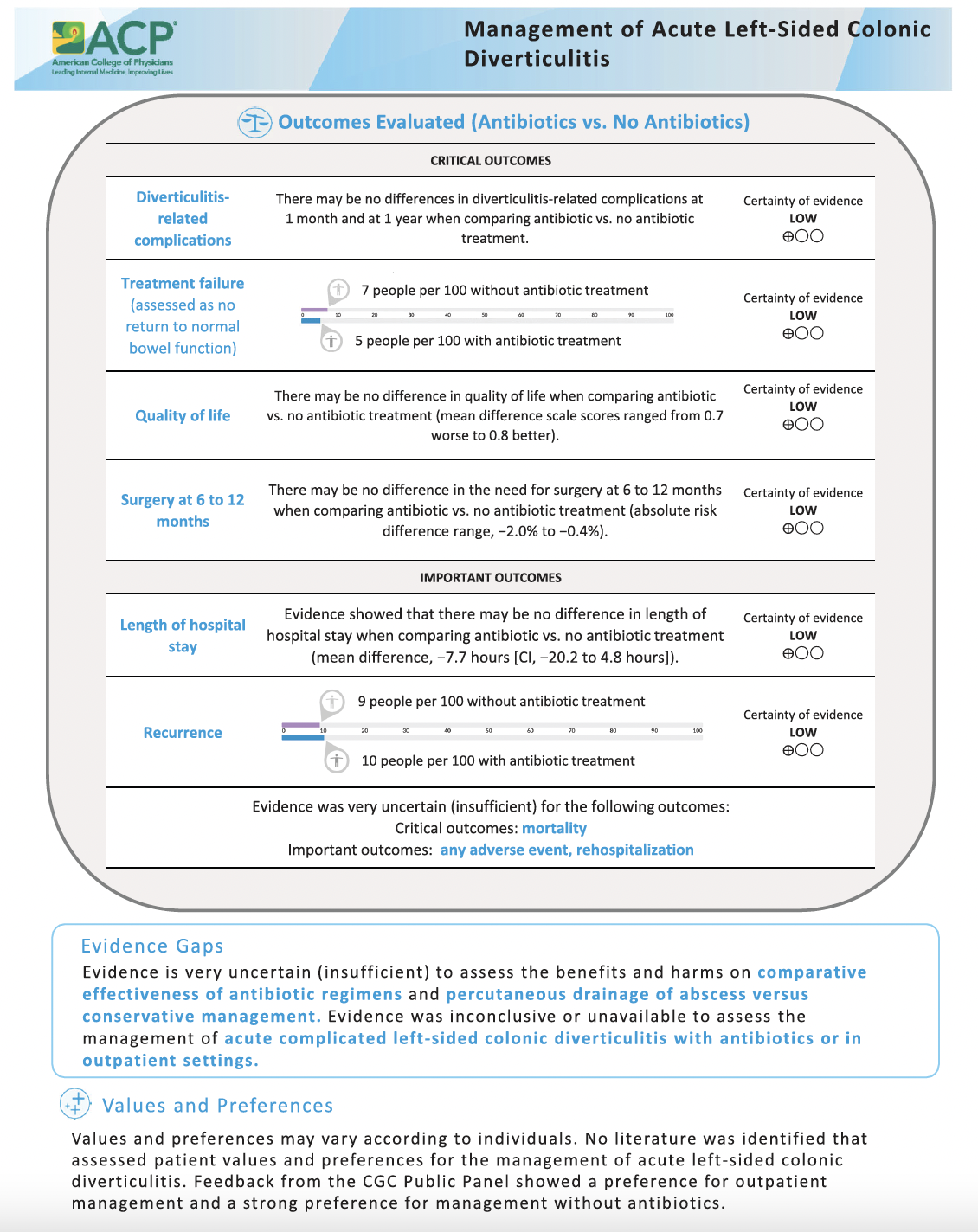
Low-certainty evidence (5 studies) comparing antibiotics Rx with no Abx showed no significant differences in need for surgery at 6-12mo (ARD -2.0% to 0.4%), complications at 1mo (1.1% vs 1.8%) and 1yr (2.1% vs 4.0%), and quality of life at 3/6/12/24months. These studies mostly enrolled immunocompetent adults with uncomplicated left ACD, however. There was insufficient evidence re: comparing Abx regimens for all important outcomes and durations of therapy. There was a strong preference to treatment without Abx by patient participants.
Harms/Adverse Effects of Recommendations: There is always a risk of detecting clinically insignificant findings, which may lead to different diagnostic/treatment decisions that may not be relevant for morbidity, mortality or patient quality of life.
Potential harms from CT scanning include radiation exposure, detecting incidental findings that are clinically irrelevant, and contrast dye reactions.
Studies typically didn’t report on harms, adverse events or side effects of infections (nosocomial, other), Abx usage (eg. C. Diff infections, resistance) or adverse procedure events (eg. bleeding, catheter infections).
Barriers to Uptake: Geographic distance from definitive care and caregiver supports may be an important consideration in decisions re: imaging, therapies and out-patient care. The costs of a contrast CT abdo were considerably variable based on US Medicare vs uninsured patient status ($USD 56-94 vs. $USD 580-4900). There was no summarized evidence relevant to the following PROs: progression to complicated ACD/mortality, return to normal bowel function, missed work/employment/school, and opioid misuse.
Facilitators of Uptake: The majority of included studies were conducted in ED settings, increasing the generalizability of findings to ED ACD patients.
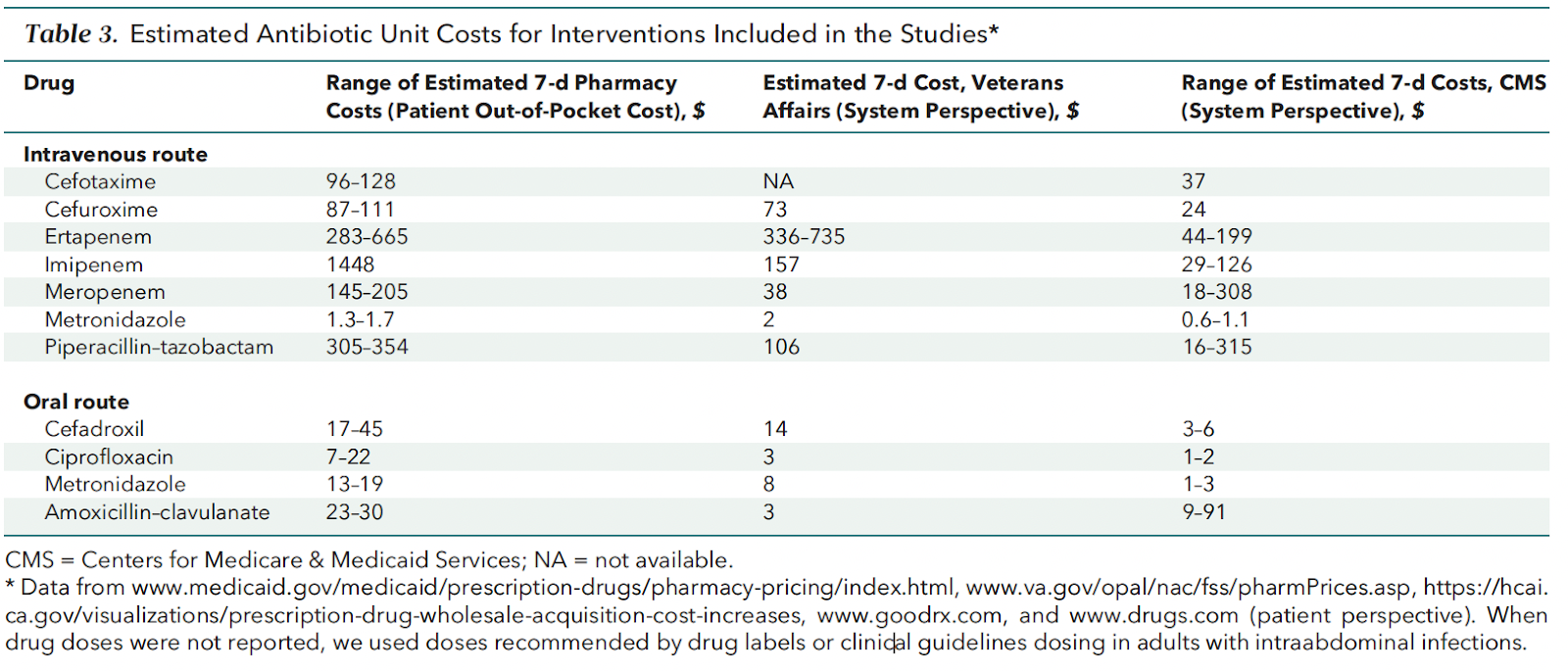
There are absolute cost savings for treating ACD patients as outpatients vs admission (generally 1/3 cost). Table 3 showed the relative Abx-costs for IV vs oral Abx treatment routes; oral Ciprofloxacin was the cheapest oral agent listed for patient out-of-pocket costs.
Non-Abx care of “select” patients focuses on supportive care to reduce bowel inflammation (analgesia, hydration, bowel rest). Select patients for non-Abx care = immunocompetent, uncomplicated left ACD, no SIRS/sepsis criteria, not medically frail/needing hospitalization for other reasons, have supportive social/family supports, and can follow-up with outpatient supervision. This decision will likely be the most contentious for ED physicians discharging patients with surgical follow-up, and should likely be made in conjuction with follow-up surgeons and patients/caregivers.
In the absence of accessible abdominal CT scan, it is reasonable to consider abdominal US or MRI scans to confirm ACD diagnosis. Clinicians should err on the side of imaging if there is risk of ACD progression to complicated disease; these include symptoms >5days duration, systemic comorbidities, high WBC > 13.5 or CRP level >140mg/L, or CT signs of perforation, GI bleeding, obstruction (vomiting), abscess/phlegmon or a longer inflamed colon segment (cutoff?).
CPG Quality/ Trustworthiness Standards
Amalgamated from AGREE-II/NEATS instruments.
| Quality/Trustworthiness Domain | |
| The clinical practice guideline (CPG) discloses and states explicitly its funding source. | ✔ |
| Financial conflicts of interest of guideline development group (GDG) members have been disclosed and managed. | ✔ |
| The CPG development group includes all of the relevant multidisciplinary stakeholders, including clinicians, methodologists and patients/caregivers. | ✔ |
| The CPG objectives, health questions, scope of relevant providers and target recipients of care are clearly defined. | ✔ |
| Values/preferences of patients, caregivers, advocates and/or the public with experience with the clinical disease management has been sought/integrated into CPG development (reported clearly). PROs listed in Table 1. | ✔ |
| The search strategy for evidence is thoroughly developed and described. | ✔ |
| The criteria for selecting relevant studies/evidence are clearly described. | ✔ |
| The quality, strengths and limitations of the body of evidence are clearly described (e.g., GRADE, Cochrane, etc.). Summaries of evidence tables are provided. Yes (in accompanying systematic review). | ✔ |
| The health benefits, side effects, and risks were considered in formulating the recommendations. | ✔ |
| There is an explicit approach linking the evidence to formulate the recommendations. | ✔ |
| The strength of recommendations is clearly reported, including confidence in underlying evidence. | ✔ |
| Recommendations are clear and unambiguous, and easily identified in the CPG publication. | ✔ |
| Different options for management for managing the health questions are clearly presented. | ✔ |
| Experts externally reviewed the guideline prior to its publication. | ✔ |
| The CPG describes a procedure to update the guideline, and provides advice, tools and/or clinical pathways for easy adoption/adaptation into practice. Expires within 5yrs. No tools to facilitate uptake. | ? |
| The CPG describes barriers and facilitators to implement recommendations. | X |
| Performance metrics for monitoring implementation of recommendations for audit/feedback have been defined appropriately. | X |
| Resource implications for implementing CPG recommendations have been discussed. Multiple economics databases searched for relevant resources/costing information. | ✔ |
Funding: (Reported) Funding provided from the ACP operating budget.
Conflicts of Interested: (Reported) Declared and managed. One panelist recused from voting and authorship due to advisory board status with an ongoing trial.
**EVIDENCE Profiles from supporting Systematic Review (Balk et al, Annals Int Med 2022)
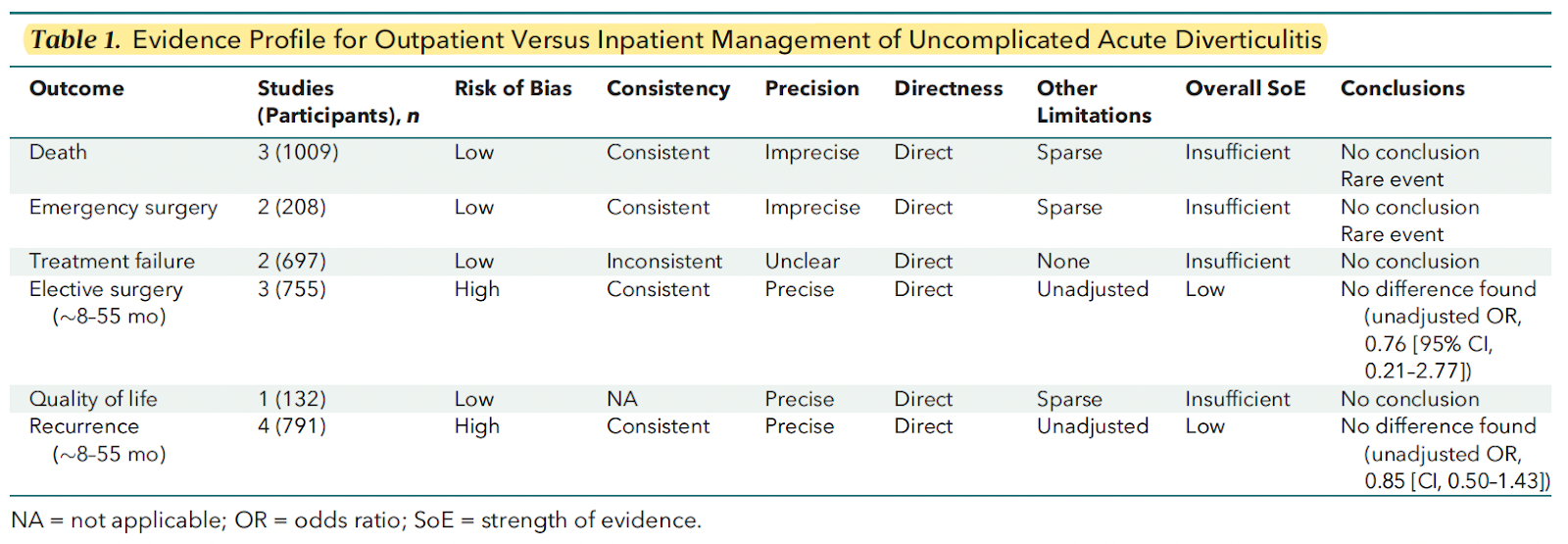
Table 1 Summary: The evidence comparing out-patient vs. in-patient management of uncomplicated ACD is sparse and inconclusive to push a Recommendation in either direction. Shared decision-making with patients, caregivers and follow-up surgeons should be undertaken to generate an individual care plan.
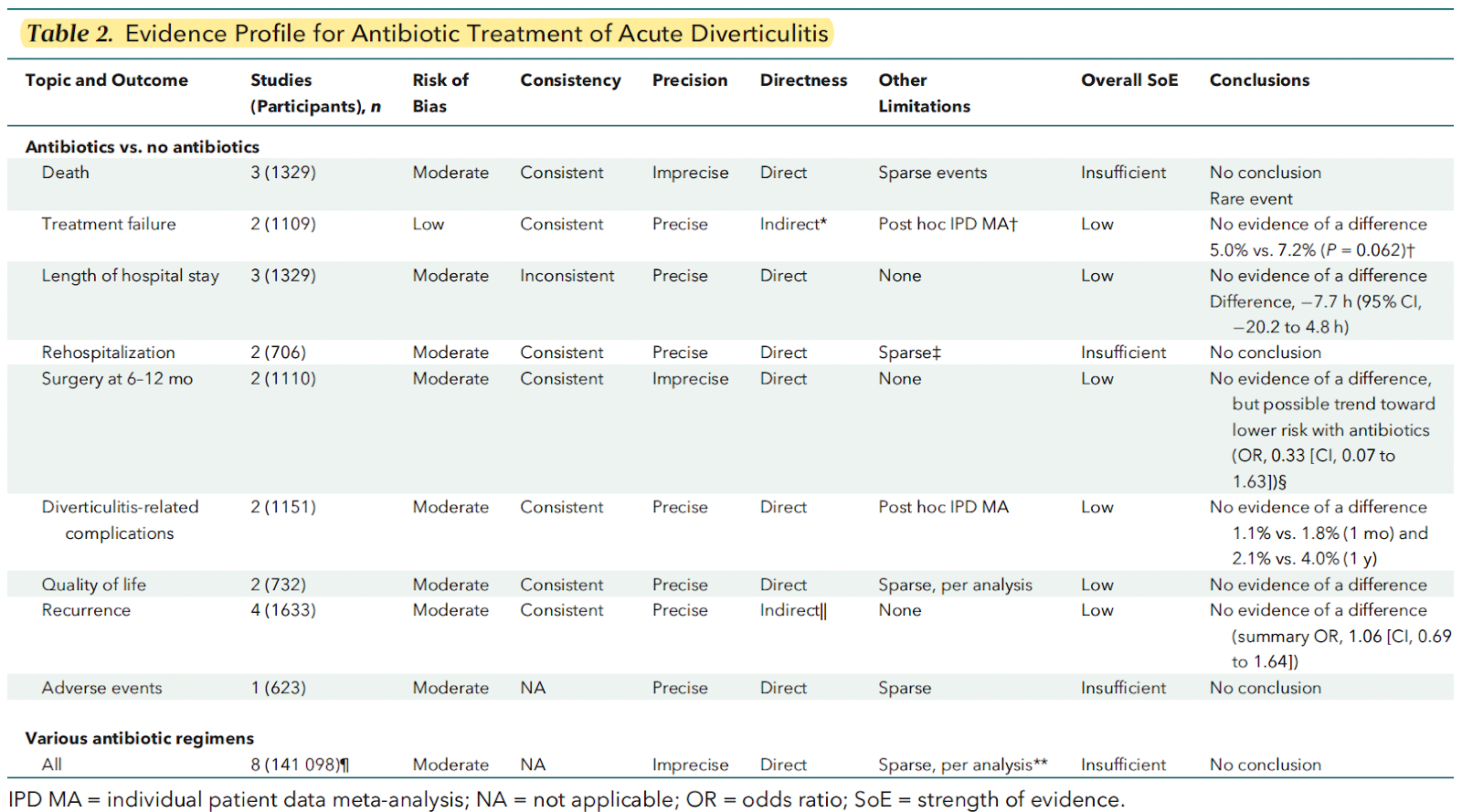
Table 2 Summary: Sparse evidence found no difference in risks for treatment failures, elective surgery, ACD recurrence, hospital length-of-stay, quality of life or ACD complications. There was insufficient evidence presented to inform comparative risks of death, rehospitalizations, or Abx-related adverse events (largely because of rare events).