MONTHLY FEATURE CPG SOPR SUMMARY
CPG Citation: Apfelbaum JL, Hagberg CA, Connis RT, Abdelmalak BB, Agarkar M, Dutton RP, Fiadjoe JE, Greif R, Klock PA, Mercier D, Myatra SN, O’Sullivan EP, Rosenblatt WH, Sorbello M, Tung A. 2022 American Society of Anesthesiologists (ASA) Practice Guidelines for Management of the Difficult Airway. Anesthesiology 2022; 136(1): 31-81.
Downloadable at: DOI: 10.1097/ALN.0000000000004002 PMID: 34762729
Scope of Guideline: Guidelines are intended for adult and pediatric patients with either anticipated or unanticipated difficult airways, obstetric patients, intensive care (ICU) patients, and critically ill patients. Not applicable for patients at risk of aspiration, nor physiologic (not anatomic) difficult airways.
Inclusion: All airway management and anesthetic care delivered in in-patient settings, including the Emergency Department (and other critical care settings).

Summary download – click![]()
Exclusion: Pre-hospital settings, and individuals who do not deliver anesthetic care or perform airway management.
Key Words: Difficult airway, emergency department.
Key Recommendations: Each recommendation is accompanied by the “strength” of recommendation and the level of evidence (LoE) supporting that recommendation
**Strength of Recs (LoE) NOT explicitly reported in publication!!
| Recommendations |
| 1) Evaluation for Difficult Airway (DA): The most responsible airway personnel should confirm medical, surgical, environmental and anesthetic factors that can influence patient airway outcomes. Get historical information as needed from patient, family, medical records, etc. Complete a physical exam to determine any anatomic predictors of difficult airways. Determine a risk of needing advanced airway equipment (eg. bronchoscope, surgical airway). |
| 2) DA Preparation: Have all equipment for advanced/emergency airway interventions on hand; consider preparing a “Difficult Airway” cart with appropriate training. Ensure proper positioning and supplement oxygen use prior to initiating DA interventions. |
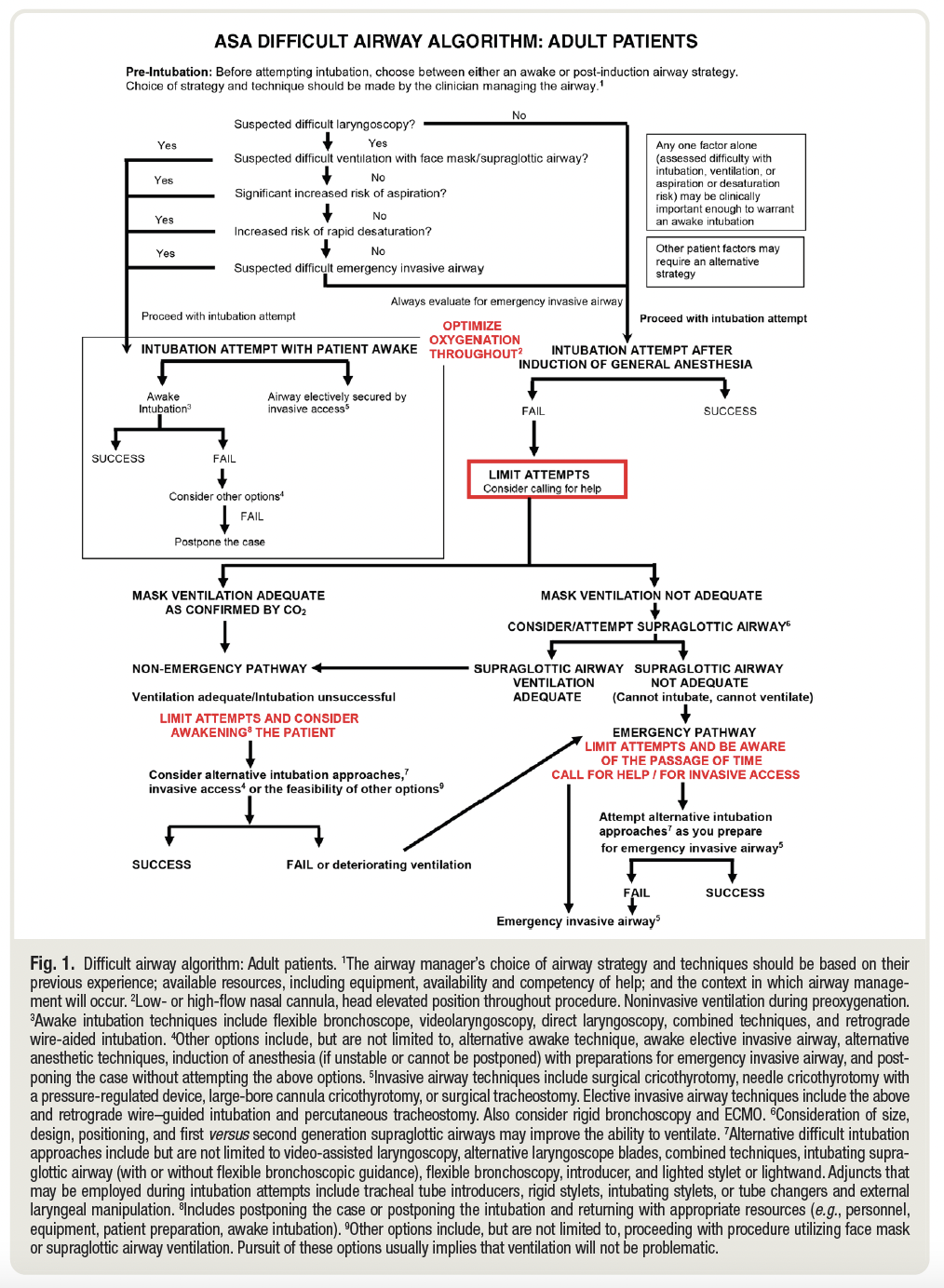
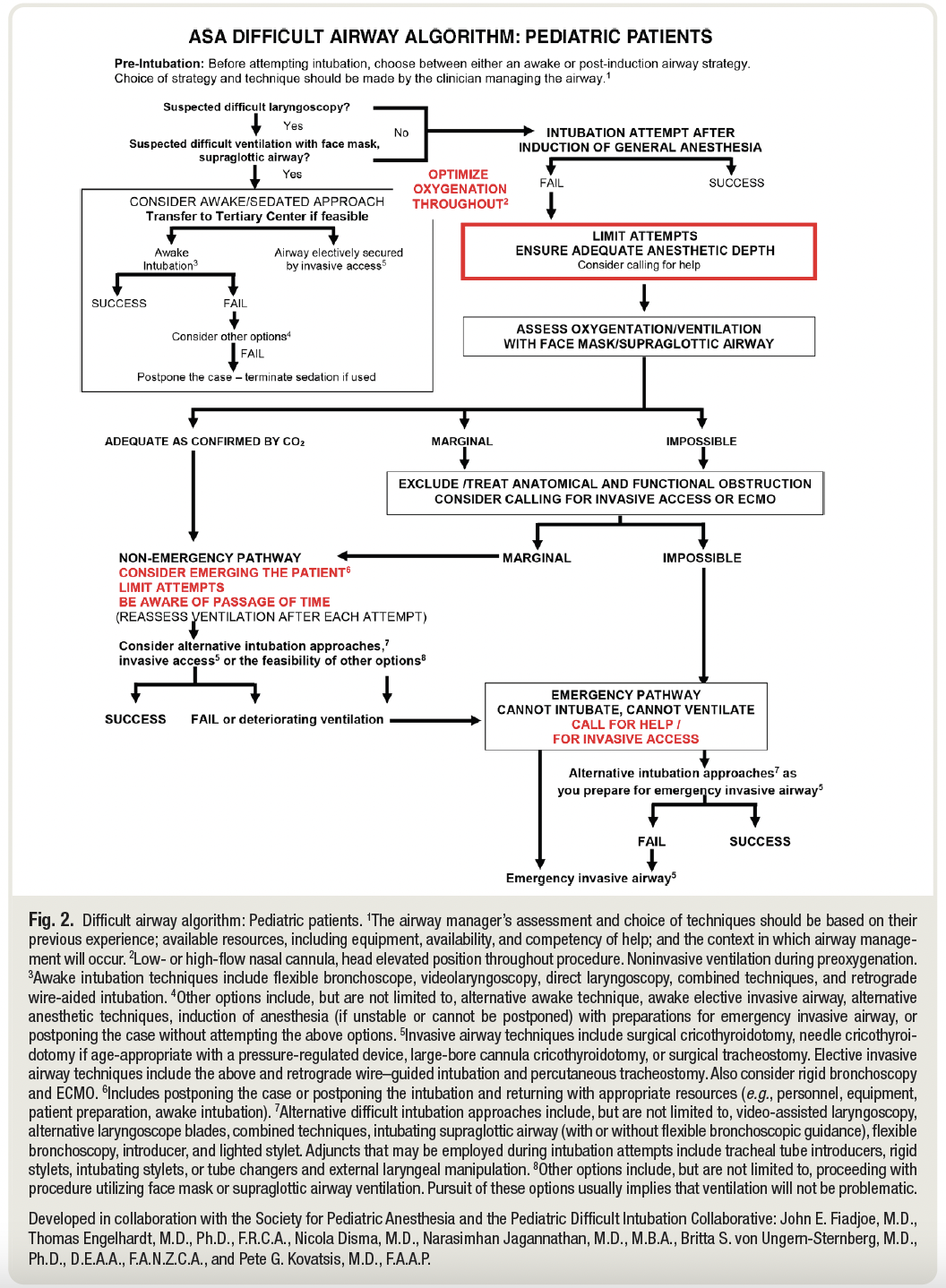
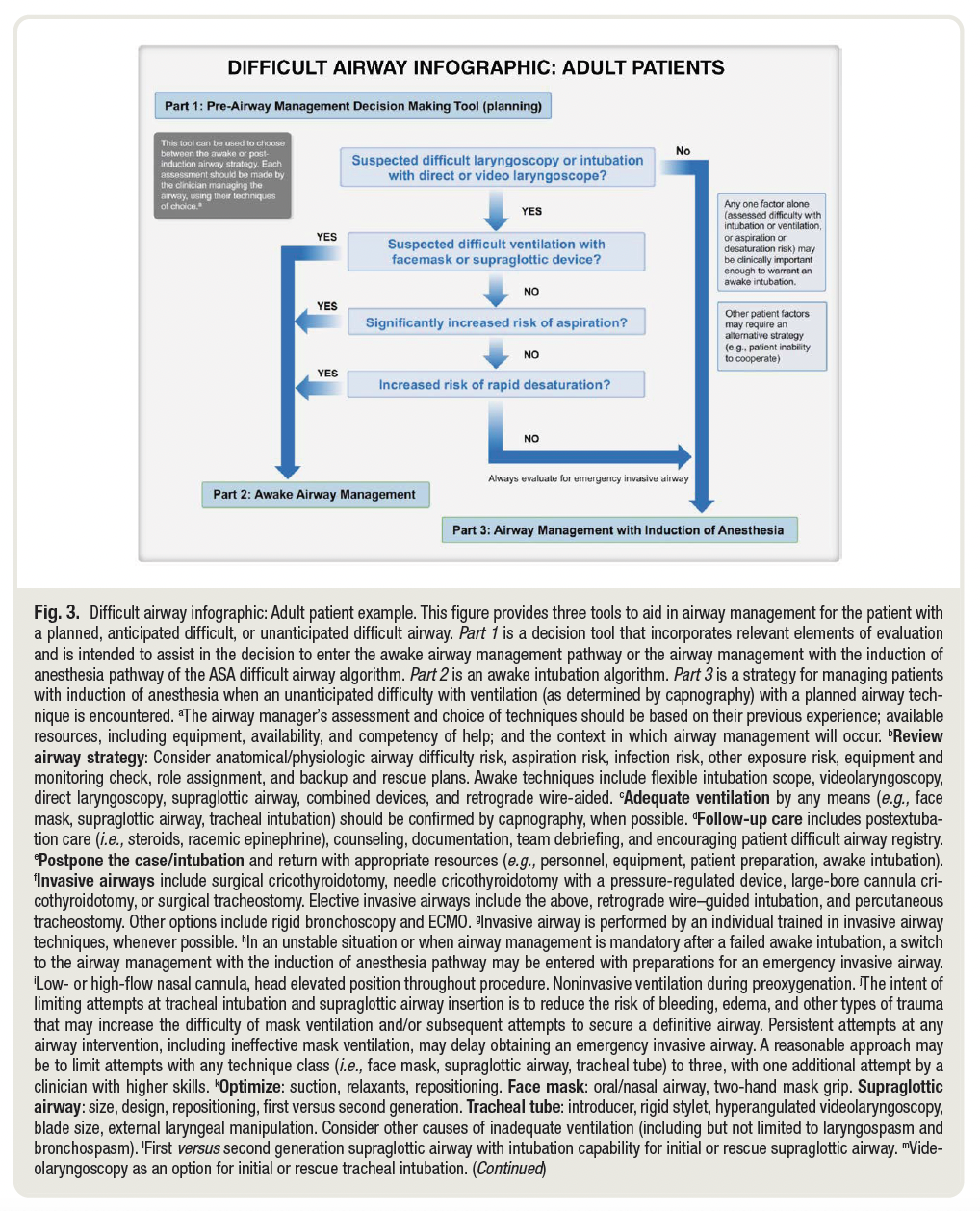
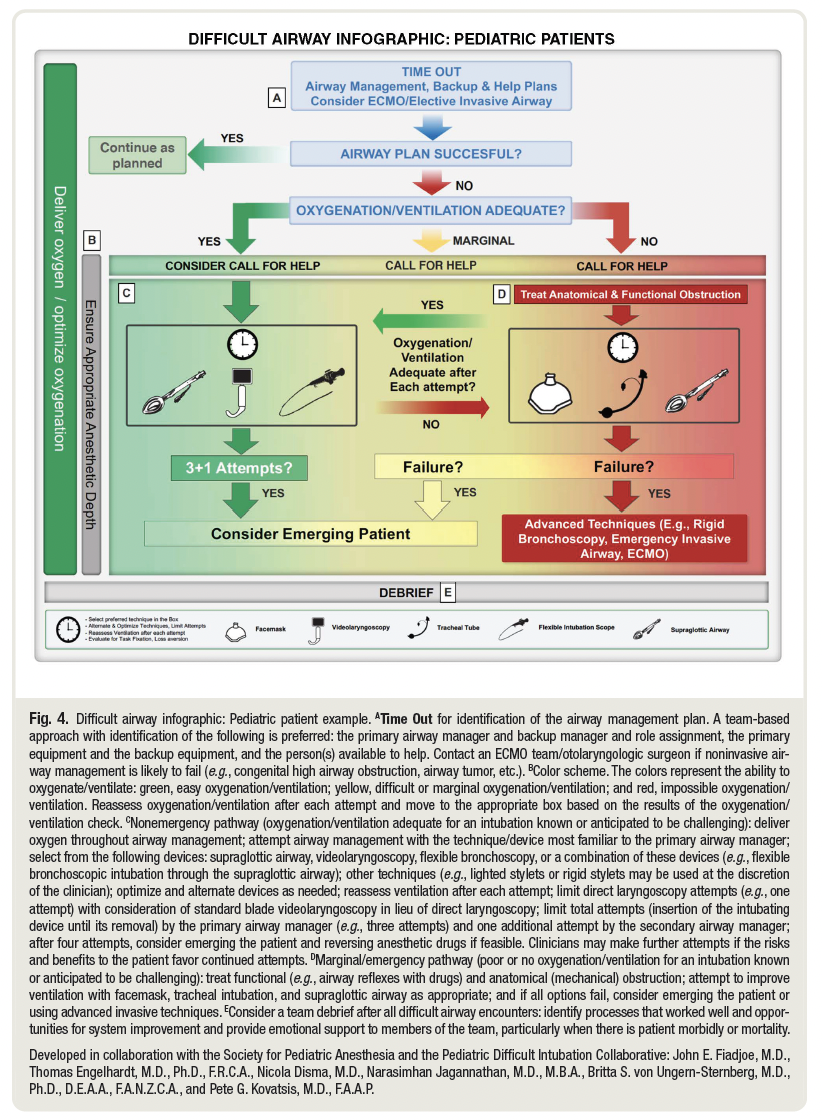
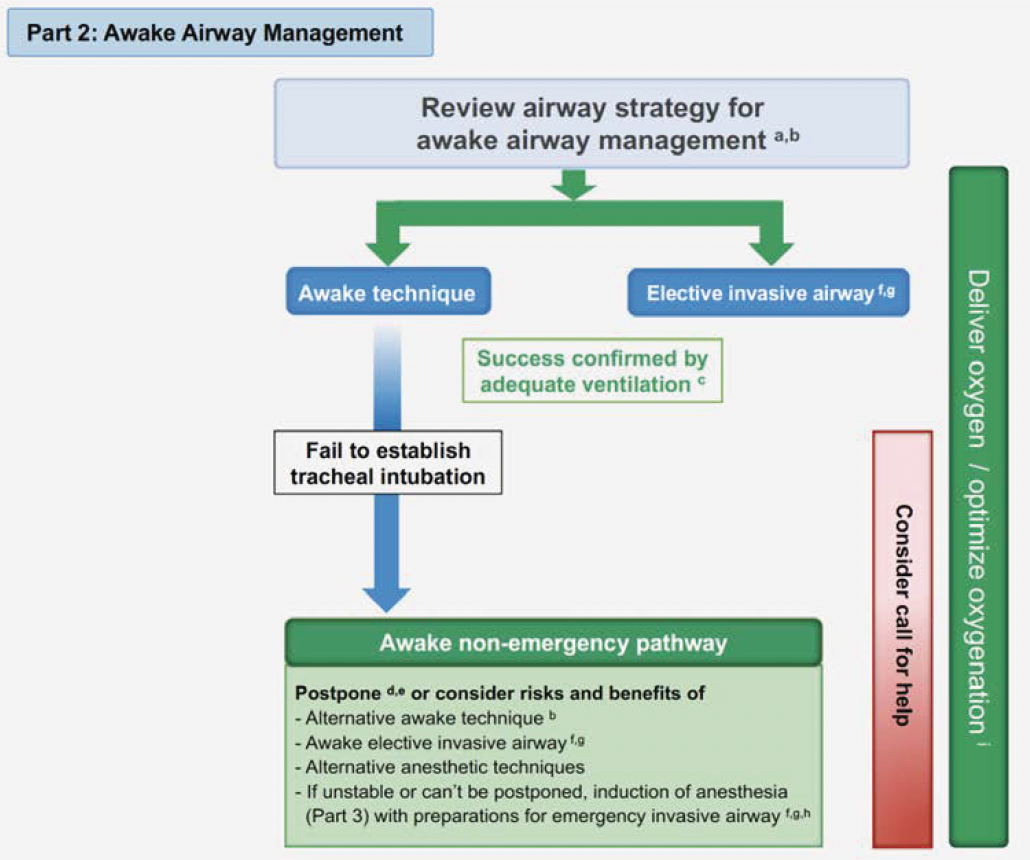
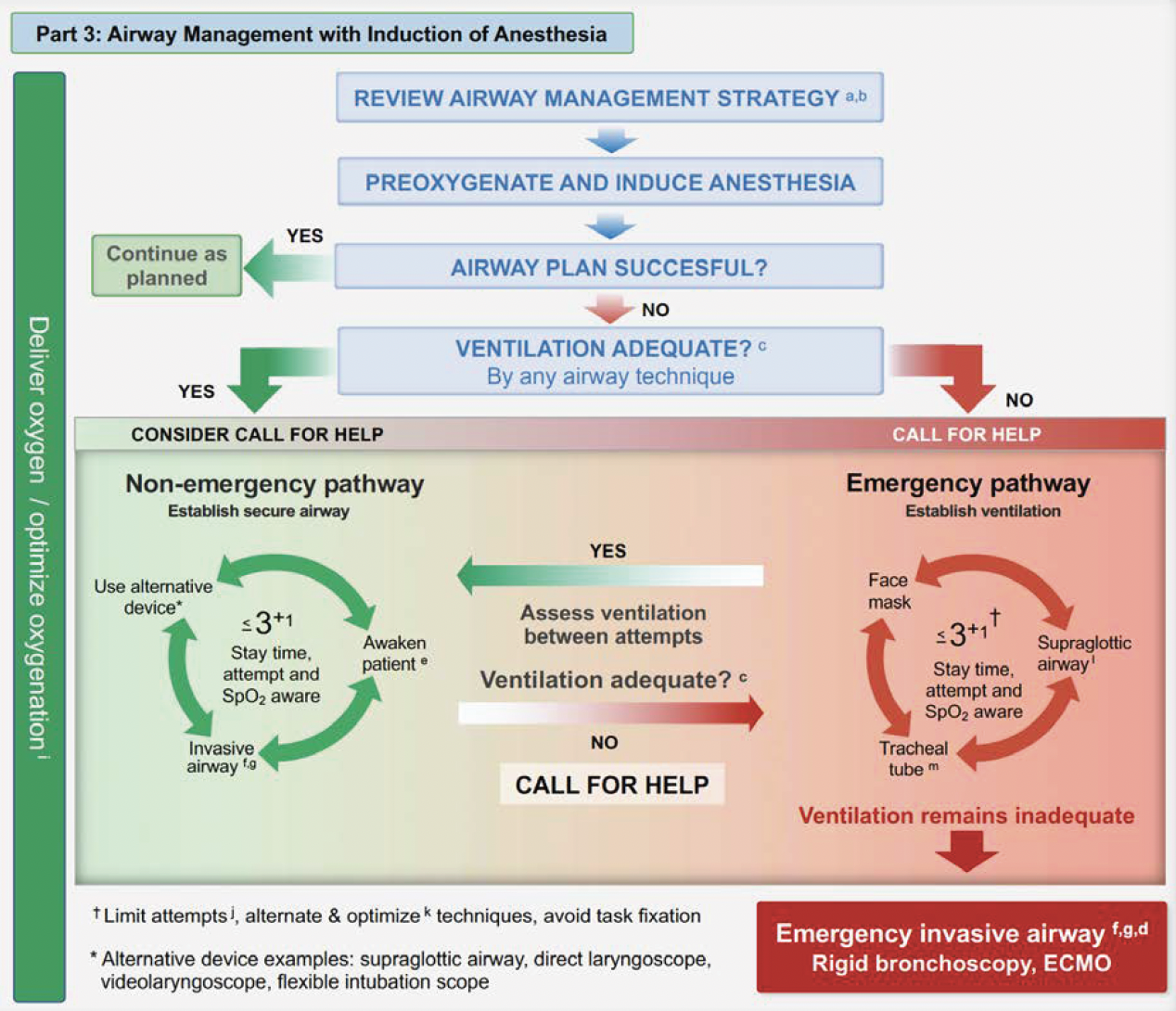
| 3) Anticipate DA: Identify step-wise strategies for awake intubation, DA patients who can be adequately ventilated, DA patients who can’t be ventilated/intubated, and invasive rescue airway procedures. When appropriate, start with awake intubations if: a) difficult ventilation (face mask/supraglottic airway), (b) increased risk of aspiration, (c) DA patient is likely incapable of tolerating a brief apneic episode, or (D) there is expected difficulty with emergency invasive airway rescue. Anticipate need to vary interventions for pediatric or uncooperative patients. Be ready to used combined techniques for DA interventions as clinically warranted. Limit the number of unsuccessful intubation attempts to avoid trauma. Be wary of the passage of time with repeated attempts; monitor oxygen saturation throughout the procedure. Ensure oxygenation between attempts with BVM ventilation. |
| 4) Unanticipated DA: Call for help as needed. Optimize oxygenation (BVM). Determine appropriateness of non-invasive vs invasive interventions. For invasive airway Rx, ensure proper training/experience for airway personnel, and complete the airway intervention as expeditiously as possible. |
| 5) Confirmation of Tracheal Intubation: Use capnography/end-tidal CO2 monitoring to confirm endotracheal intubation. |
Benefits of Recommendations: Recs were rated through an international survey of airway experts worldwide, using a 5-pt Likert scale; the majority of Recs received “Strongly Agree” or “Agree” endorsements. These Recs update prior information with more recent relevant evidence, and address different topics from prior publications. Enacting some/most of these Recs should improve DA outcomes in the ED.
Harms/Adverse Effects of Recommendations: There are no clear linkages between the reviewed evidence, and subsequent Recs for each topic category. This can make it hard to differentiate those Recs that may be “Strong” (with higher supporting LoE) vs. those that are “Weak/Conditional” (lower LoE).
Facilitators of Uptake: A properly constructed Difficult Airway program for the ED (with multidisciplinary stakeholder inputs), with appropriate education content, hands-on/simulation training, and credentialing can optimize the performance of ED staff in real-time DA situations.
Clinical algorithms are provided for adoption/adaptation into the ED workplace.
Barriers to Uptake: Guidelines do not provide any materials for education, training nor credentialling. Emergency Departments looking to operationalize these Recs would need to develop a de novo training program for such (or adapt those of others).
There are no quality improvement performance indicators based on “Strong” Recs offered for implementing the algorithms presented.
CLINICAL COMMENTARY: Difficult airways are to be anticipated and prepared for in every emergency setting, and is understandably a core competency for all EM practitioners. Like every skill, however, lack of practice will erode skills, so constant maintenance of competency is essential. This can be achieved through simulation training/credentialing in your institution, in collaboration with other relevant stakeholders (eg. ED nursing, anesthesia, ENT, respiratory techs, etc.).
Creating and launching an institutional Difficult Airway training program can reduce unplanned airway incidents in most large and smaller community hospitals.
Funding: (Reported) Support provided solely by the ASA (pg 51).
Conflicts of Interested: (Reported) Multiple authors had various disclosures of academic grants, and industry support. Management of those with various conflicts was not clearly disclosed.
Key References:
- Orebaugh SL. Difficult Airway Management in the Emergency Department. J Emerg Med 2002; 22(1): 31-48.
- Brown NS, Chirico J, Hollidge M, Randall J. Clinical leadership in reducing risk: Managing patient airways. Healthcare Manage Forum 2019;32(2):92-96. doi: 10.1177/0840470418810678.
- Kornas RL, Owyang CG, Sakles JC, et al. Evaluation and Management of the Physiologically Difficult Airway: Consensus Recommendations From Society for Airway Management. Anesth Analg 2021 Feb 1;132(2):395-405. doi: 10.1213/ANE.0000000000005233.
CPG Quality/ Trustworthiness Standards
Amalgamated from AGREE-II/NEATS instruments.
| Quality/Trustworthiness Domain | |
| The clinical practice guideline (CPG) discloses and states explicitly its funding source. | ? |
| Financial conflicts of interest of guideline development group (GDG) members have been disclosed and managed. Disclosed YES; management not reported. | ? |
| The CPG development group includes all of the relevant multidisciplinary stakeholders, including clinicians, methodologists and patients/caregivers. No patients/caregivers. | ? |
| The CPG objectives, health questions, scope of relevant providers and target recipients of care are clearly defined. | ✔ |
| Values/preferences of patients, caregivers, advocates and/or the public with experience with the clinical disease management has been sought/integrated into CPG development (reported clearly). No patient values/preferences reported. | ? |
| The search strategy for evidence is thoroughly developed and described. | ✔ |
| The criteria for selecting relevant studies/evidence are clearly described. | ✔ |
| The quality, strengths and limitations of the body of evidence are clearly described (e.g., GRADE, Cochrane, etc.). Summaries of evidence tables are provided. | ✔ |
| The health benefits, side effects, and risks were considered in formulating the recommendations. | ✔ |
| There is an explicit approach linking the evidence to formulate the recommendations. No | X |
| The strength of recommendations is clearly reported, including confidence in underlying evidence. “Strong” vs “Conditional/Weak” Recs not stated clearly. | X |
| Recommendations are clear and unambiguous, and easily identified in the CPG publication. Appendix 1. | ✔ |
| Different options for management for managing the health questions are clearly presented. | ✔ |
| Experts externally reviewed the guideline prior to its publication. Survey external experts. | ✔ |
| The CPG describes a procedure to update the guideline, and provides advice, tools and/or clinical pathways for easy adoption/adaptation into practice. No update plan, but clinical pathways provided. | ✔ |
| The CPG describes barriers and facilitators to implement recommendations. | X |
| Performance metrics for monitoring implementation of recommendations for audit/feedback have been defined appropriately. | X |
| Resource implications for implementing CPG recommendations have been discussed. | X |