MONTHLY FEATURE CPG SOPR SUMMARY
Date: February 2021
CPG Citation: Hatten BW, Cantrill SV, Dubin JS, Ketcham EM, Runde DP, Wall SP, Wolf SJ. Clinical
Policy: Critical Issues Related to Opioids in Adult Patients Presenting to the Emergency Department. Annals Emerg Med 2020; 76:e13-e39. https://doi.org/10.1016/j.annemergmed.2020.06.049
Downloadable at: https://www.acep.org/patient-care/clinical-policies/opioids/ (free online access)
Scope of Guideline: Physicians working in Emergency Departments
Inclusion: Adult patients presenting for unscheduled acute care settings.
Exclusion: Pediatric patients.
Key Words: Opioid, pain, opioid use disorder (OUD), buprenorphine.
Summary download – click ![]()
CPG Questions:
1) In adult patients experiencing opioid withdrawal, is ED-administered buprenorphine as effective for the management of opioid withdrawal compared with alternative management strategies?
2) In adult patients experiencing an acute painful condition, do the benefits of prescribing a short course of opioids on discharge from the ED outweigh the potential harms?
3) In adult patients with an acute exacerbation of noncancer chronic pain, do the benefits of prescribing a short course of opioids on discharge from the ED outweigh the potential harms?
4) In adult patients with an acute episode of pain being discharged from the ED, do the harms of a short concomitant course of opioids and muscle relaxants/sedative-hypnotics outweigh the benefits?
Key Recommendations: Each recommendation is accompanied by the “strength” of recommendation and the level of evidence (LoE) supporting that recommendation
| Recommendations | Strength (LoE) |
| FOR Clinical Action 1. When possible, treat opioid withdrawal in the ED with buprenorphine or methadone as a more effective option compared with nonopioid-based management strategies such as the combination of a2- adrenergic agonists and antiemetics. | Level B |
| NEUTRAL Clinical Action 1 .Preferentially treat opioid withdrawal in the ED with buprenorphine rather than methadone. | Level C |
| 2. Preferentially prescribe nonopioid analgesic therapies (nonpharmacologic and pharmacologic) rather than opioids as the initial treatment of acute pain in patients discharged from the ED. | Level C |
| AGAINST Clinical Action 1. Do not routinely prescribe opioids to treat an acute exacerbation of noncancer chronic pain for patients discharged from the ED. Nonopioid analgesic therapies (nonpharmacologic and pharmacologic) should be used preferentially. | Level C |
| 2. Do not routinely prescribe opioids to treat an acute exacerbation of noncancer chronic pain for patients discharged from the ED. Nonopioid analgesic therapies (nonpharmacologic and pharmacologic) should be used preferentially. | Level C (Consensus) |
CLINICAL COMMENTARY:
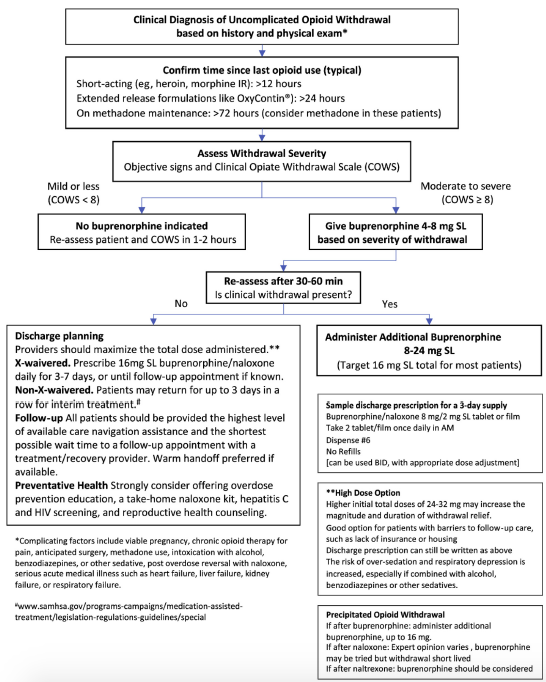
Q1. Regarding ED-buprenorphine initiation, there is growing evidence supporting this practice for patients experiencing opioid withdrawal, especially with expedited follow-up with addiction services.
Suboxone is the preferential ED-initiation option, as it safer than methadone, with less risk of toxicity due to mixed receptor partial agonism (and ceiling effect on respiratory depression).
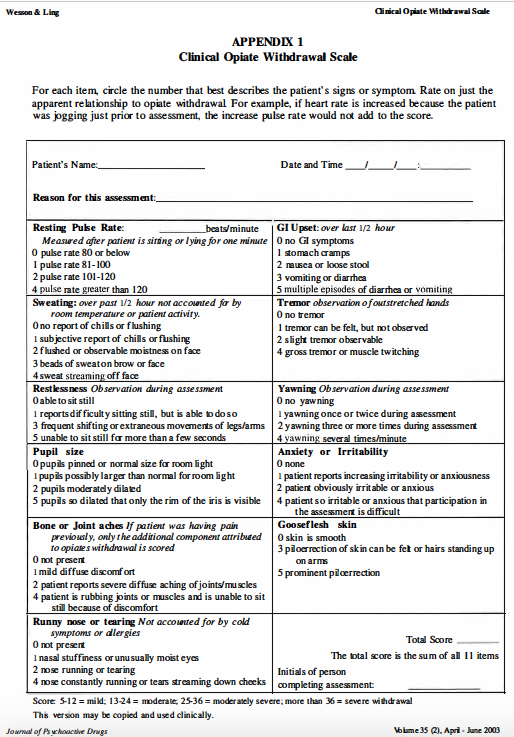
There is an easy to follow clinical algorithm to assess opioid withdrawal and initiate ED buprenorphine provided in the Policy. Users should also familiarize themselves with the COWS (Clinical Opioid Withdrawal Scale) tool in order to measure severity of opioid withdrawal (similar to CIWA scoring for alcohol withdrawal).
Opioid withdrawal symptoms may vary with opioids consumed (eg. heroin within 12hrs, methadone within 30hrs). It is uncomfortable, but not life-threatening.
Symptomatic control of opioid withdrawal may also include the following:
- Pain control: Non-opioid analgesics
- Nausea/vomiting: Anti-emetics
- Diarrhea: loperamide
- Mixed withdrawal symptoms: alpha-2-adrenergic agents (clonidine, lofexidine) may be helpful for these. This is based on limited reviews in the literature (Gowing et al, Cochrane 2009; Gottlieb et al, Annals Emerg Med Syst Rev Snapshot 2017). Benzodiazepines may be useful for muscle cramps, anxiety and catecholamine excess, but this must be a careful ED consideration in the context of SUD assessment, and concomitant mental health concerns/medications use.s
Of note, initiation of ED buprenorphine should happen with patients in active withdrawal. Use of buprenorphine in nonwithdrawal patients using opioids may induce withdrawal,
It is critical for patients being initiated with buprenorphine (or methadone) to be referred/ confirmed for follow-up in a rapid addiction assessment medicine (RAAM) clinic, so as not to lose continuity of opioid agonist Rx initiated in the ED. Ideally this should be an integrated continuity of initiation/referral program that is pre-established with your ED.
Additional support info for ED buprenorphine initiation is linked at: http://www.drugabuse.gov/ed-buprenorphine and http://www.medicine.yale.edu/edbup.
Q2. Treating acute pain problems in the ED should ideally be done with non-opioids if possible. There is high quality recent evidence/guidance supporting the role of NSAIDs & acetaminophen in acute musculoskeletal non-low back pain conditions (Busse et al, Annals Int Med 2020). For primarily neuropathic pain conditions, treatment with gabapentinoids, TCAs, duloxetine or cannabinoids can be effective and opioid-sparing in the ED.
Treating ED acute pain effectively yet safely is an appropriate patient-oriented goal, and opioids could have a role in managing acute pain and preventing transition (wind-up) to chronicity (Feizerfan 2015). Appropriate screening of ED acute pain patients for risk of long-term opioid use is warranted, although the usual opioid dependency screening tools (eg. SOAPP, COMM, Opioid Risk Tool) have not been validated in ED settings, or proven to be not useful in ED screening. Having said that, just as every person who has a drink of alcohol does not become an alcoholic, every opioid consumer does not eventually become an opioid addict, especially if using a short duration of medication in the acute phase. Informed shared-decision making (SDM) with the acute pain patient is paramount to achieve an appropriate treatment goal, and should be documented accordingly. Of note, using an Alternatives to Opioids (ALTO) first strategy has been shown to reduce opioid prescribing yet maintain patient satisfaction (Duncan et al, Am J Emerg Med 2019).
There is a small but non-zero risk of prolonged use in opioid-naïve patients after receiving an initial opioid script in the ED (Riva et al, Annals Int Med 2020). As such, multiple academic and government regulatory guidance documents promote opioid avoidance in acute pain situations, followed by a short course of low-potency opioids (ideally ≤3 days, no longer than 7days), with a total morphine equivalence of <90-100mg total for the discharge script. If using non-morphine choices, consult online calculators to determine conversion factors to morphine-equivalence (MEQ). Where possible, jurisdictional PDMP’s should be consulted prior to providing potential duplicate scripts. It is also important to ensure that all opioids are stored safely (in order to minimize loss/diversion), and all potential common adverse effects are addressed (eg. constipation). Stopping and returning unused opioids is also important to avoid inadvertent unauthorized use (eg. household children), or other diversion concerns. For example, it has been shown that many ED opioid scripts are neither completely filled nor consumed, resulting in an excess number of unused pills available for misuse/diversion (Daoust et al, 2018).
Of note, Daoust et al (Acad Emerg Med 2019) that some patients who are still using opioids 3mo after the index visit may be using legitimately for ongoing pain problems, but not misusing for non-pain purposes. In a related study, they found that patients on a “severe” pain arc 14days after ED visit may be associated with higher ED discharge pain severity & opioid use, but further detailed risk stratification factors are not yet determined (Daoust et al, Annals Emerg Med 2019).
In summary, there is a role for potentially providing opioids for the treatment of ED acute pain, but this would be ideally after offering non-opioid alternatives first, and then providing a limited course of lower-potency opioids if needed.
Q3. For acute exacerbations of chronic non-cancer pain (CNCP), ED physicians should offer non-opioid analgesia instead of altering/augmenting opioids. Many jurisdictions may restrict the number of physicians who can prescribe to a single patient, and these are frequently monitored in jurisdictional prescription drug monitoring programs (PDMPs). There is also a potential benefit of reducing progression to OUD with incremental opioids consumed. The counter-balancing harm might include leaving acute pain untreated in CNCP patients. Increased risk factors for developing OUD include concurrent mental health disorders, alcohol and other substance use disorders (AUD, SUD). Further long-term opioid use was associated with ED opioid scripts longer than 5 days, and ongoing use past 30days.
Overall, this Policy recommendation suggests that even a short course of acute opioids for CNCP has risks that outweigh any negligible/nominal benefits.
Q4. There is a confirmed risk of prescribing opioids in patients with other centrally-acting agents, like benzodiazepines and muscle relaxants (increased risk of respiratory depression), although these statements are based on a sparse base of lower-quality evidence. Congruent with discussions above, it is preferred to use other therapeutic alternatives that are not necessarily psychoactive, or at risk of negative drug interactions; these may be limited, however. A thorough review of medications is needed before prescribing any risky medications in ED, including review of all psychoactive agents (eg. Bzds, muscle relaxants, anti-depressants, analgesics, etc.), before considering any opioid scripts upon discharge. All discussions should also be documented on the clinical chart.
Prior Guideline Recommendations/Relevant Evidence:
This Policy does not update questions from the 2012 Policy (use of state prescription drug monitoring databases, opioid prescribing for acute low back pain, nor use of US short-acting Schedule II vs III opioids). This Policy also excludes commentary on opioid use for specific pain conditions (eg. acute headache, addressed in 2019 Headache Policy). Finally, this policy doesn’t address naloxone prescribing for ED opioids with at-risk patients being discharged.
There are multiple recent guidance documents and evidence reviews that address various elements of opioid prescribing in acute pain conditions, but most of the evidence in these summaries are weak/inconclusive, or indirect at best. A lack of ED opioid advice in high-profile guidelines has been noted previously (Upadhye et al, 2019).
Disclaimer (if stated): None
Funding reported: Project support by ACEP
Grading System Used: ACEP Clinical Policies ABC/I-II-III framework.
IOM Guideline “Trustworthiness” Checklist
| Rating Domain | Rating (Good/Fair/Poor) |
| Establishing transparency | Good |
| Managing conflict of interest in CPG development group | Good |
| Group composition (range of stakeholders involved) | Fair (no patient/public stakeholders) |
| Critical evaluation of supporting evidence | Fair; searches limited to English articles, electronic databases and bibliography searches, expert inputs |
| Framing recommendations based on supporting evidence | Good |
| Clear articulation of recommendations | Good |
| External review by relevant stakeholders/organizations* | Good |
| Updating schedule | Fair (last CPG 2012) |
| Implementation issues | Poor |
*Internal/external inputs sought from: emergency physicians, clinical pharmacists, Am Acad Clinical Toxicology, ABEM, Am Soc Addiction Med, ACEP Medical-Legal committee and ACEP Quality & Patient Safety committee.