MONTHLY FEATURE CPG SOPR SUMMARY
CPG Citation: Ohle R, Yan JW, Yadav K, et al. Diagnosing acute aortic syndrome: a Canadian clinical practice guideline. CMAJ. 2020 Jul 20;
192(29):E832-E843.
Downloadable at: https://www.cmaj.ca/content/192/29/E832
Summary download – click ![]()

Scope of Guideline: This is a guide for emergency medicine physicians, family physicians, internists, radiologists, vascular surgeons, cardiothoracic surgeons, critical care physicians, patients and decision-makers to select a diagnostic strategy for acute aortic syndrome (excluding ruptured or leaking aortic aneurysms) that is most likely to yield a diagnostic result with the minimum number of diagnostic tests and radiation exposure.
Inclusion/Exclusion: Adults (≥ 18 years) with suspected AAS. AAS Definition = intramural dissection, hematoma or penetrating ulcer. Exclusions: Pregnancy; recent (< 24 hr) cocaine use, leaky/ruptured aortic aneurysms.
Key Recommendations: Each recommendation is accompanied by the “strength” of recommendation and the level of evidence (LoE) supporting that recommendation
| Recommendations | Strength (LoE) |
| FOR Clinical Action 1a. Assess risk of AAS in patients with non-traumatic chest, abdominal, back pain and/or perfusion deficit, syncope, interarm blood pressure differential > 20 mm Hg or systolic blood pressure > 180 mm Hg. AAS risk factors include connective tissue and aortic valve diseases, recent aortic manipulation, thoracic or abdominal aortic aneurysm and history of AAS. High-risk AAS pain and physical exam features include abrupt onset, severe, tearing or migrating pain and new aortic regurgitation, pulse deficit, neurological deficit, hypotension or pericardial effusion respectively. | Strong (Low) |
| 4a. If high (> 5%) AAS probability, start with ECG-gated CT. | Strong (Moderate) |
| NEUTRAL Clinical Action 3a. If moderate (0.5 to 5%) AAS probability, use D-dimer to rule out. If D-dimer positive, use ECG-gated CT. | Conditional (Low) |
| 4b. If high (> 5%) AAS probability, do not perform D-dimer testing. | Conditional (Moderate) |
| AGAINST Clinical Action 1b. Assess AAS probability as low (≤ 0.5%), moderate (0.5 to 5%) or high (> 5 %). | Conditional (Low) |
| 2. If low (≤ 0.5%) probability of AAS, do not test. | Conditional (Low) |
| 3b. If moderate (0.5 to 5%) AAS probability and D-dimer or ECG-gated CT negative, no further testing. | Conditional (Low) |
Key Decision Aids:
Clinical features of AAS (increase pre-test probability): pain (chest/abdo/back), clinical perfusion deficits (CNS, ACS, limb, mesenteric), or BP differentials (>20mmHg [common in 20% general population], sBP >180mmHg)
Acute Aortic Syndrome (AAS) Score:
| Risk Assessment Category | Characteristics | |
| Risk Factors = aortic valve dz, family history AAS, connective tissue dz, recent aortic manipulation; Known aortic aneurysm* | None Any non-aneurysmal risk factors Aortic aneurysm* | 0 1 2 |
| Pain Features = tearing/ ripping sensation, severe/worst ever, onset abrupt/ thunderclap, migrating or radiating | No high-risk pain features 1-2 high-risk pain features 3+ high-risk pain features | 0 1 2 |
| Physical Exam (PE) findings = pulse deficits, neurologic deficits, new aortic insufficiency (auscultation/POCUS, hypotension/ pericardial effusion (POCUS) | No high-risk PE findings Any high-risk PE finding | 0 2 |
| Alternate Diagnosis | Suspicion for alternate diagnosis** Unsure AAS most likely diagnosis | -1 0 1 |
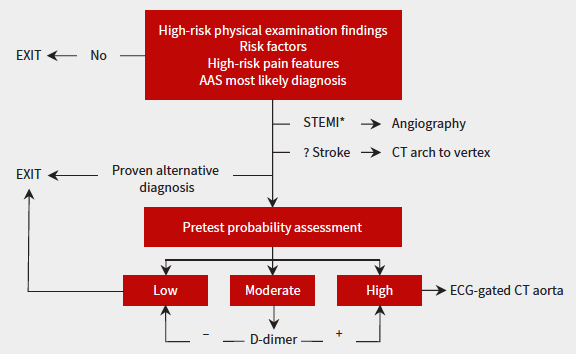
0: LOW risk probability (<0.5%) = no further investigations needed
1: MODERATE risk probability (0.5-5%) = D-Dimer testing
2+: HIGH risk probability (>5%) = ECG-gated CT aortogram
** Suspected alternate Dx: If suspected ACS with concomitant AAS, consider CXR, POCUS and D-Dimer testing in addition to usual ACS evaluations. If suspected/confirmed PE, hold anticoagulation until AAS is ruled out.
Decision Algorithm:
CLINICAL COMMENTARY:
Acute aortic syndrome (AAS) is a rare (1/2000 ED presentations for acute chest/back pain, overall incidence 3/100000 persons), but is a time-dependent emergency with a linear mortality increase of 2% per hour of diagnostic delay. There is a 25% miss rate for AAS in initial ED presentations, and misdiagnosis rates up to 38%, highlighting the need consider and rule out this rare yet dangerous diagnosis in the ED.
The need to avoid diagnostic error/misses are counter-balanced by the need to avoid unnecessary CT imaging, which increases radiation exposures, contrast dye exposures, ED length of stay, and resource costs. Furthermore, the discovery of incidental findings contributes to patient stress/anxiety and may lead to future investigations (unnecessary?).
Finally, there is a medicolegal risk associated with missed AAS (Upadhye 2012). Case findings show a multitude of alternative diagnoses with missed AAS, and summary judgments caution ED physicians to consider the AAS diagnosis in higher-risk presentations, and abnormal ECG/physical exam findings.
This CPG has many strong features that are supportive of ED practice. The authorship group is primarily ED physicians (community, academic) who have extensive clinical experience and methodological expertise to create this document. The use of GRADE methodology is thorough and explicitly reported, which increases confidence in the readers. A simple scoring tool and clinical decision aid is presented, which should be easy to follow for ED physicians (both await future validation); there is planning to create an online decision support tool, which should further facilitate use of both the score and algorithm. There are implementation and performance measures suggested to facilitate new and ongoing quality improvement/PDSA cycles. There is also a commitment to update within 5yrs if new evidence warrants revisions of recommendations.
Limitations: There is incomplete reporting of patient involvement during the CPG development process, although patients were engaged in this project.
Prior Guideline Recommendations/Relevant Evidence:
This CPG updates and augments recommendations from prior AHA and ESC documents, and quantifies the various clinical assessment elements into a specific scoring tool and decision-making algorithm.
Funding reported: Alternate Funding Plan Innovation grant from the Northern Ontario Academic Medical Association. No influence in CPG development process, nor creating recommendations.
METHODOLOGY:
Grading System Used: GIN/McMaster Checklist, GRADE
IOM Guideline “Trustworthiness” Checklist
| Rating Domain | Rating (Good/Fair/Poor) |
| Establishing transparency | Good |
| Managing conflict of interest in CPG development group | Good |
| Group composition (range of stakeholders involved) | Good |
| Critical evaluation of supporting evidence | Good |
| Framing recommendations based on supporting evidence | Good |
| Clear articulation of recommendations | Good |
| External review by relevant stakeholders/organizations | Good |
| Updating schedule | Good; planned for 5yrs |
| Implementation issues | Good |
Barriers/Facilitators to Implementation: (determined by qualitative interviews of diverse population of EM physicians)
| Barrier | Facilitator |
| Rationale/use of D-Dimer in AAS algorithm | Education, online decision aids |
| Decision aid not in alignment with current practice/physician understanding of risk factors | Education, online decision aids |
| Complexity of suggested decision aid | Education, online decision aids |
Suggested Performance Measures for Audit/Feedback:
- Proportion of missed AAS cases
- Time to diagnosis of AAS
- ED disposition times
- Proportion of patients getting a D-Dimer test
- Proportion of patients receiving CT aorta
- Proportion of patients transferred elsewhere for imaging/consultation