MONTHLY FEATURE CPG SOPR SUMMARY
CPG Citation: Smith MD, Fee C, Mace SE, Maughan B, Perkins JC, Kaji A, Wolf SJ. Clinical Policy: Critical Issues in the Management of Adult Patients Presenting to the Emergency Department with Community-Acquired Pneumonia (CAP). Annals Emerg Med 2021; 77: e1-e57. https://doi.org/10.1016/j.annemergmed.2020.10.024.
Downloadable at: https://www.acep.org/patient-care/clinical-policies/community-acquired-pneumonia/ (free PDF version)
Scope of Guideline: Physicians working in the ED who evaluate/treat CAP
Inclusion: Adult ED patients with a Dx of CAP. CAP defined is as an acute pulmonary parenchymal infection (new infection), usually bacterial that are treatable with anitbiotics (Abx). Causes may be community-, hospital- or ventilator-acquired.
Exclusion: Pregnant, pediatric patients
Key Words: Community-acquired pneumonia, decision aids, biomarkers, intravenous antibiotics
Summary download – click ![]()
Key Questions:
- In the adult ED patient diagnosed with community-acquired pneumonia, what clinical decision aids can inform the determination of patient disposition?
- In the adult ED patient with community-acquired pneumonia, what biomarkers can be used to direct initial antimicrobial therapy?
- In the adult ED patient diagnosed with community-acquired pneumonia, does a single dose of parenteral antibiotics in the ED followed by oral treatment versus oral treatment alone improve outcomes?
Key Recommendations: Each recommendation is accompanied by the “strength” of recommendation and the level of evidence (LoE) supporting that recommendation
| Recommendations | Strength, LoE |
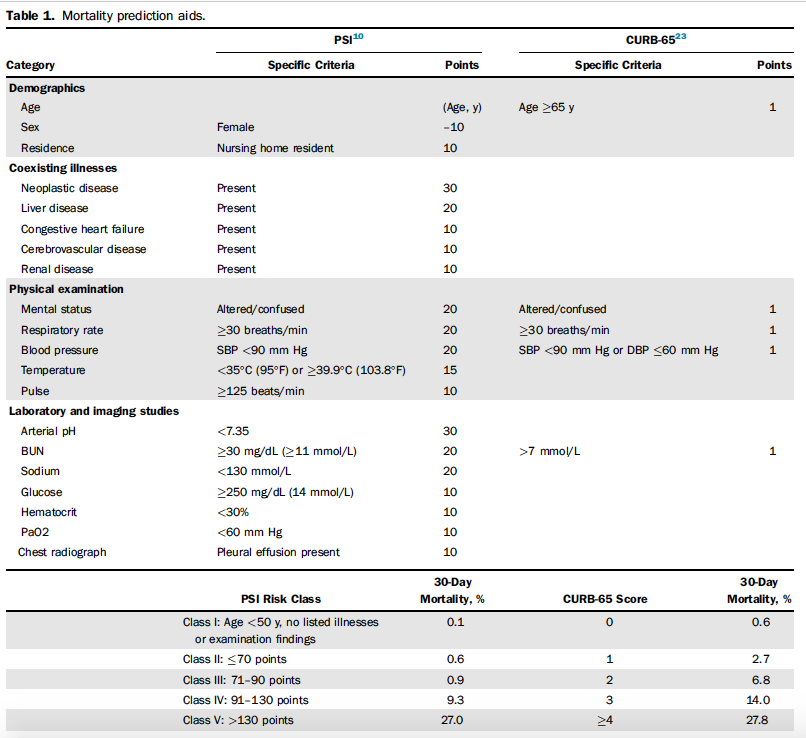
| FOR Clinical Action Q1. The Pneumonia Severity Index (PSI) and CURB-65 decision aids can support clinical judgement by identifying patients at low risk of mortality who may be appropriate for outpatient treatment. PSI is supported by a larger body of evidence and is preferred by other society guidelines (ATS/IDSA 2019 guidelines). | Level B |
| NEUTRAL Clinical Action Q1. Use CAP clinical decision aids in conjunction with physician clinical judgment in the context of each patient’s circumstances when making disposition decisions. Q1. Among patients not receiving vasopressors or mechanical ventilation, use the 2007 IDSA/ATS Minor Criteria rather than mortality prediction aids such as the PSI or CURB-65 to help establish which patients are most appropriate for care based in an ICU setting. Q3. Given the lack of evidence, the decision to administer a single dose of parenteral antibiotics prior to oral therapy should be guided by patient risk profile and preferences. | Consensus Consensus Level C |
| AGAINST Clinical Action Q1. Do not routinely use biomarkers to augment the performance of clinical decision aids to guide the disposition of ED patients with CAP. Q2. Do not rely upon any current laboratory test(s), such as procalcitonin and/or C-reactive protein (CRP), to distinguish a viral pathogen from a bacterial pathogen when deciding on administration of antimicrobials in ED patients who have CAP. | Consensus Level C |
Benefits of recommendations:
Q1. Use of clinical decision aids (PSI > CURB65) can help stratify low-risk patients for outpatient Rx. Both tools have been validated for ED use, although PSI seems to have a stronger supportive evidence base (better NPV and AUC for 30d mortality prediction); CURB65 is faster to calculate in ED, and less lab variables needed. They may also help determine which sick admitted CAP patients may need to be in ICU (2007 IDATS/ATS Minor Criteria; reaffirmed 2019). It is likely, however, that admitting services (Medicine, ICU) will be making disposition decisions for sick admitted patients, so the practical utility of these scores is less certain?
Q2. Not using routine biomarkers can avoid unnecessary painful needles for patients, needlestick injuries for staff, and expensive lab testing that doesn’t change management.
Q3. Improved patient autonomy/satisfaction/compliance with treatment plan, as mutually agreed upon with shared decision-making (SDM).
Harms of recommendations:
Q1. There may other elements for unsafe discharge (immunocompromise, social barriers, unable to tolerate oral Abx) not captured by the PSI/CURB65 that may disqualify their use. Physician judgment and shared decision-making with the patient are always warranted. No biomarker is sufficiently validated in ED to warrant use in replacing or in conjunction with CDA’s above to merit inclusion/use in testing. Furthermore, no biomarker has been validated for mortality prediction in ED CAP patients. (Biomarkers evaluated: procalcitonin, MR-proADM [midregional pro-adrenomedullin]).
Q2. There are no harms associated with avoiding unnecessary biomarker tests for ED CAP.
Q3. There are no harms by promoting SDM Rx plans with your patient. There are considerable harms from a single-dose ED Abx intervention followed by outpatient oral Abx. These include painful needles to patients, needlesticks to staff, increased ED length of stay, materials/staffing costs, and complications of IV access (superficial phlebitis, pain, local infection). This practice contravenes general principles of Abx stewardship, and is not evidence-based. In borderline patients who are “somewhat” sick who may not warrant admission but a period of observation, then initial IV Abx loading with concomitant oral meds may be warranted.
CLINICAL COMMENTARY:
This policy updates evidence/recommendations on current management of ED CAP. CAP is the 8th leading cause of death in the USA, and most common reason for hospital admission (1.5 admissions/year, cost $USD 11,000-51,000 per admit). In Canada, CAP remains one of the most common cause of infection death (Statscan), and is the leading cause of infection death in lower/middle-income countries (LMICs; Michaud 2009). Worldwide, WHO 2020 concluded that lower respiratory tract infections were the #4 cause of death, after CV disease, stroke and COPD. Due to the sheer volume of CAP illnesses, morbidity and mortality, it behooves ED physicians to have an evidence-based approach to risk-stratifying patients who need testing, admission and treatment to avoid excessive illness/deaths, and to yet be prudent resource stewards to optimize high-value care.
It is important that ED physicians be aware of and align clinical practices with the best evidence-based recommendations available for ED CAP management, ideally produced by EM organizations.
Prior Guideline Recommendations/Relevant Evidence:
This policy updates the prior ACEP Policy from 2009. The 2009 Policy addressed unnecessary routine blood cultures in ED admitted low-risk CAP patients, but still indicated for high-risk admissions. This is unchanged here.
The ATS/IDSA 2019 CPG updates CAP recommendations (available free at https://www.atsjournals.org/doi/full/10.1164/rccm.201908-1581ST).
The NICE (UK) 2019 CPG update focuses mostly on antibiotic prescribing recommendations for CAP. Clinicians probably should best refer to local antibiograms, resistance patterns and prescribing recommendations for CAP Rx in their own communities/hospitals. This document is available at: https://www.nice.org.uk/guidance/ng138.
A CADTH Rapid Review (2020) of ED CAP CPG’s found that both PSI and CURB65 are useful decision aids for making admission decisions, but that PSI is favoured by ATS/IDSA 2019, whereas CURB65 is favoured by UK NICE. This report is freely accessible at: https://cadth.ca/management-patients-presenting-pneumonia-emergency-department-guidelines.
Disclaimer (if stated): N/A
Funding reported: ACEP. No role in collecting/analyzing literature, nor crafting recommendations.
Grading System Used: ACEP Level A/B/C and Evidence I/II/III system (originally from Schriger et al, 1993).
IOM Guideline “Trustworthiness” Checklist
| Rating Domain | Rating (Good/Fair/Poor) |
| Establishing transparency | Good |
| Managing conflict of interest in CPG development group | Good (None reported) |
| Group composition (range of stakeholders involved) | Poor (no patient/public stakeholders) |
| Critical evaluation of supporting evidence | Fair (limited search)* |
| Framing recommendations based on supporting evidence | Good; usual use of A/B/C and I/II/III ACEP framework |
| Clear articulation of recommendations | Good |
| External review by relevant stakeholders/organizations | Good** |
| Updating schedule | Good? Suggest every 3yrs (last done 2009) |
| Implementation issues | Poor (no performance metrics for QI monitoring, audit/feedback) |
* Search limited to English language articles, electronic databases with some subsequent bibliography searches from recent articles (identified by committee members). No mention of grey literature searches (conference abstracts, theses, etc.).
** Draft review by ER physicians (via ACEP membership), clinical pharmacists, internal medicine specialists, American Thoracic Society, Infectious Disease Society of America, ACEP Medical-Legal and Quality/Patient Safety committees.