MONTHLY FEATURE CPG SOPR SUMMARY
CPG Citation: Mahmud E, Dauerman HL, Welt GFP, Messenger JC, Rao SV, Grines C, Mattu A, Kirtane AJ, Jauhar R, Meraj P, Rokos IC, Rumsfeld JS, Henry TD. Management of Acute Myocardial Infarction During the COVID-19 Pandemic; A Position Statement from SCAI, ACC & ACEP. JACC 2020, 76(11): 1375-1384. https://doi.org/10.1016/j.jacc.2020.04.039
Downloadable at: https://onlinelibrary.wiley.com/doi/10.1002/ccd.28946
Scope of Guideline: Not specified; presumably intended for all practitioners involved with ACS/STEMI care, including ED, medical/cardiology, EMS transport and regional cath lab personnel. Mostly aimed at US health system care.
Inclusion: Not specified
Exclusion: Not specified

Summary download – click ![]()
Key Words: myocardial infarction, COVID19, catheterization
Key Recommendations: This document represents consensus recommendations by experts from the Society for Cardiac Angiography & Interventions (SCAI), American College of Cardiology (ACC) and American College of Emergency Physicians (ACEP).
| Recommendations | Strength, LoE |
| FOR Clinical Action For definite STEMI, rapid PCI is still standard of care. Assume all patients are potentially COVID+ and protect patient/staff accordingly.Patients should be masked, or if intubated, usual protective filters applied.If available/high sensitivity/reliable, deploy ultra-rapid ED COVID testing to ascertain patient COVID status.Be mindful of “STEMI-mimics” that are commonly seen with COVID19 heart disease (eg. myocarditis, stress cardiomyopathy, etc.); consider ED POCUS/ECHO to determine wall motion abnormalities (WMA)Use selective consideration for OCHA survivors with STEMI who may need PCI referral (high risk of COVID transmission). | N/A |
| NEUTRAL Clinical Action If STEMI transfer to cath lab is not practical, ED staff may employ IV thrombolysis as per usual practices.If STEMI not clearly established, usual ED workup for ACS and manage accordingly. Use serial ECGs in case of delayed STEMI (then cath lab if STEMI)For OCHA survivors without STEMI, send to PCI center if ongoing hemodynamic instability or acute coronary occlusion still highly likely; get a multi-disciplinary team consensus first prior to transfer.For inter-facility transfers, EMS should avoid ED bypass; have the patient reassessed in ED first to confirm need for PCI lab, then transfer accordingly. | N/A |
| AGAINST Clinical Action Do not consider invasive interventions for STEMI for critical COVID-pulmonary illness/ICU admission with low likelihood of survival. Consider palliative strategies instead. Ideally this should be a collaborative shared decision (staff, family/caregivers, etc.).If remote STEMI receives IV thrombolysis, do NOT routinely transfer to PCI center post-lysis. Call PCI team to discuss ongoing care based on IV lysis response.Elevated troponins without STEMI are not an indication for PCI transfer; manage medically and consider non-infarction differentials (myocarditis, stress cardiomyopathy, LV strain, right heart failure, coronary spasm). Consider PCI if high GRACE/other score, or hemodynamic instability. | N/A |
Benefits of Recommendations: Primary intervention for STEMI is still standard of care, regardless of COVID status. In clear cut STEMI cases, make rapid transfer decisions for definitive intervention, with all due appropriate PPE/infection protections for all involved staff. If possible, do an ultra-rapid ED COVID test to ascertain patient COVID status.
Harms/Adverse Effects of Recommendations: There may be delays in otherwise routine interventional investigations/treatments offered to higher-risk patients as a result of needs to protect critical staff/cath labs/PPE resources in the face of unknown COVID risks. All interventions/procedures in AMI care should be considered high-risk for aerosol/droplet generation. Doing a double-check of PCI need in the recipient hospital ED exposes the receiving ED staff to potential COVID, but presumably protects the PCI facility/staff if the PCI indication is no longer present.
**Balance Benefits vs. Harms: Need for balancing the needs of prompt STEMI interventional care with infection protection risks for all parties involved with care/transport. With the advent of ultra-rapid COVID testing, the need for universal infection control/PPE utilization should become more stream-lined.
Barriers to Uptake: Reluctance of patients to attend ED with early ACS/STEMI symptoms due to COVID fears. STEMI mimicks associated with COVID19 (may require additional testing to confirm STEMI, leading to treatment delays). Inability to deploy rapid COVID testing. Reluctance to transfer STEMI patients to cath labs, esp if involving EMS transport to a regional centre (risk of multiple contaminations). Inability to coordinate detailed communication/patient planning between treatment sites. Reluctance of recipient hospital ED to consider bypass cessation and need for a re-evaluation. Reduced ICU, ventilator and ECMO capacity during COVID outbreaks.
Facilitators of Uptake: Availability of rapid COVID testing. Expedited access to ED ECHO/other modalities to differentiate STEMI mimics. Pre-written algorithms for each variation of ACS/STEMI patient usually seen in ED, with COVID modifiers.
CLINICAL COMMENTARY: The COVID pandemic has created challenges in ED care for a multitude of time-dependent emergencies, including STEMI. The logistics of managing infection control priorities, transport safety for EMS staff, and inter-facility transports for definitive PCI in the face of potential COVID spread create considerable challenges for all parties. Given the commitment to maintain rapid PCI as the STEMI standard of care, novel strategies to balance patient care and staff safety must be managed. Innovative solutions based on regional realities must be created to achieve this balance…
Prior Guideline Recommendations/Relevant Evidence: The authors tried to amalgamate usual ACS/STEMI care guidance with current realities of COVID19 infection control needs, and overburdened health systems/resources during the pandemic. Some early STEMI real-world process experiences reported in observational studies is analyzed (non-critically), and incorporated into these recommendations.
Disclaimer (if any stated): None reported.
Funding reported: None reported.
Grading System Used: None reported.
Figure 1. STEMI Care (Patient already AT PCI center)
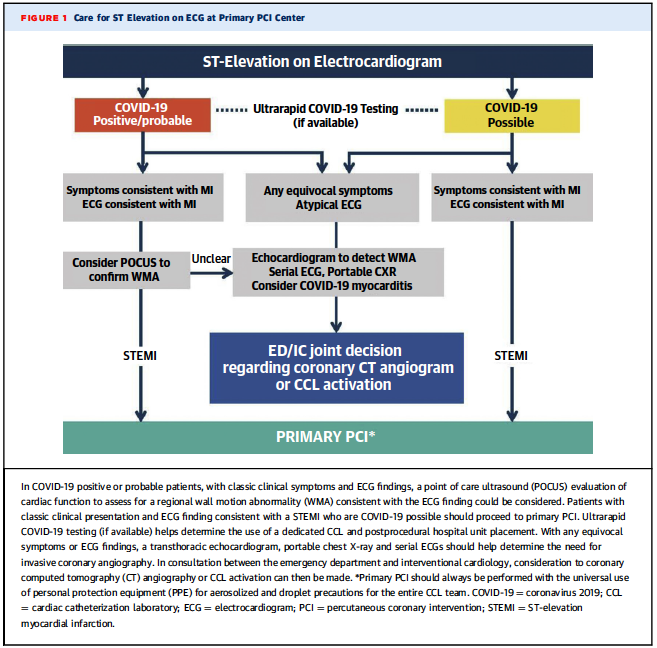
Figure 2. Field Algorithm for ACS/STEMI Patient
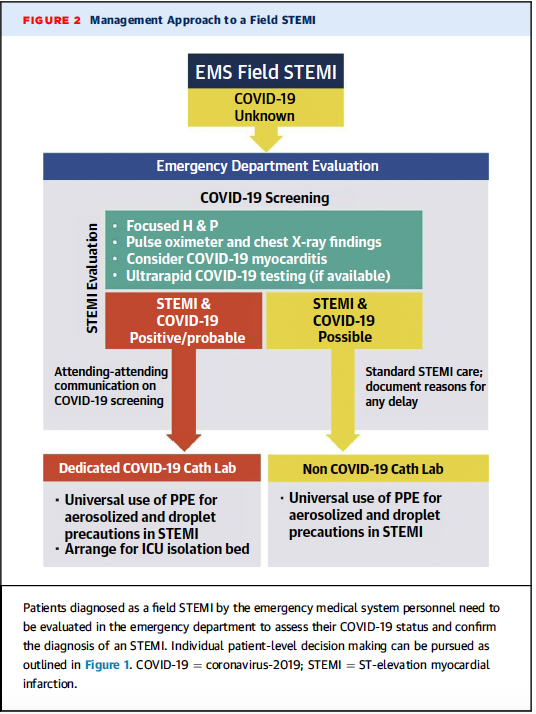
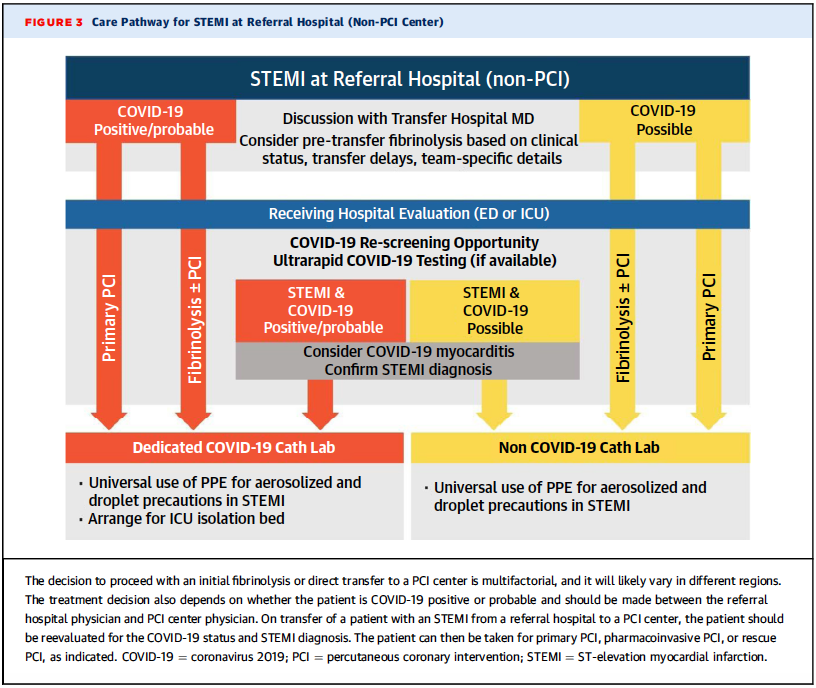
Figure 3. STEMI Patient NOT at PCI Center (may need transfer)
Institute of Medicine 2011 Trustworthiness Standards
| Rating Domain | Rating (Good/Fair/Poor) |
| Establishing transparency | Fair |
| Managing conflict of interest in CPG development group | Good; Panelists with written CoI were recused from discussing/voting on recommendations |
| Group composition (range of stakeholders involved) | Fair; all members of SCAI, ACC; 1 EM ACEP member. No patients/other stakeholders |
| Critical evaluation of supporting evidence | Poor; paucity of evidence. Observational trials reviewed (6), but no attempt at critical appraisal |
| Framing recommendations based on supporting evidence | Fair; no systematic review of evidence. Limited integration of real-world early COVID STEMI experiences |
| Clear articulation of recommendations | Good |
| External review by relevant stakeholders/ organizations | N/A |
| Updating schedule | Poor |
| Implementation issues | Good; various clinical algorithms provided, easy to follow/understand |