MONTHLY FEATURE CPG SOPR SUMMARY
CPG Citation: Gulati M, Levy PD, Mukherjee D, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/ SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines.
Circulation. 2021 Nov 30;144(22):e368-e454. PMID: 34709879
Downloadable at: doi: 10.1161/CIR.0000000000001029. Epub 2021 Oct 28.
Scope of Guideline: Guidance for the evaluation of acute or stable chest pain (or anginal equivalents), in different clinical settings, with an emphasis on diagnosing ischemic causes.
Inclusion: Numerous recommendations around the evaluation and management of chest pain.
Exclusion: No recommendations re: need/modalities of revascularization.

Summary download – click![]()
Key Words: Chest pain syndromes, angina, coronary artery disease, acute coronary syndrome, myocardial ischemia/infarction/injury, noncardiac chest pain, accelerated diagnostic pathway, clinical decision pathway, sex differences, troponins, biomarkers, shared decision-making, cardiac imaging
Key Recommendations: Each recommendation is accompanied by the “class of recommendation” and the level of evidence (LoE) supporting that recommendation.
**For brevity, only CoR1 and 3 Recs are presented, and limited to those Recs relevant for ED practice.
MACE = major adverse cardiac event
| Recommendations | CoR, LoE |
| FOR Clinical Action | |
| 1. An initial assessment of chest pain is recommended to triage patients effectively on the basis of the likelihood that symptoms may be attributable to myocardial ischemia. | CoR1, B-NR |
| 2. Chest pain should not be described as atypical, because it is not helpful in determining the cause and can be misinterpreted as benign in nature. Instead, chest pain should be described as cardiac, possibly cardiac, or noncardiac because these terms are more specific to the potential underlying diagnosis. | CoR1, C-LD |
| 3. In patients with chest pain, a focused history that includes characteristics and duration of symptoms relative to presentation as well as associated features, and cardiovascular risk factor assessment should be obtained. | CoR1, C-LD |
| 4. Women who present with chest pain are at risk for underdiagnosis, and potential cardiac causes should always be considered. | CoR1, B-NR |
| 5. In women presenting with chest pain, it is recommended to obtain a history that emphasizes accompanying symptoms that are more common in women with ACS. | CoR1, B-NR |
| 6. In patients with chest pain who are >75 years of age, ACS should be considered when accompanying symptoms such as shortness of breath, syncope, or acute delirium are present, or when an unexplained fall has occurred. | CoR1, C- LD |
| 7. Cultural competency training is recommended to help achieve the best outcomes in patients of diverse racial and ethnic backgrounds who present with chest pain. | CoR1, C-LD |
| 8. Among patients of diverse race and ethnicity presenting with chest pain in whom English may not be their primary language, addressing language barriers with the use of formal translation services is recommended. | CoR1, C-LD |
| 9. In patients with acute chest pain, it is recommended that 9-1-1 be activated by patients or bystanders to initiate transport to the closest ED by emergency medical services (EMS). | CoR1, C-LD |
| 10. In patients presenting with chest pain, a focused cardiovascular examination should be performed initially to aid in the diagnosis of ACS or other potentially serious causes of chest pain (eg, aortic dissection, PE, myopericarditis, sickle chest crisis, or esophageal rupture) and to identify complications. | CoR1, C-EO |
| 11. Unless a noncardiac cause is evident, an ECG should be performed for patients seen in the office setting with stable chest pain; if an ECG is unavailable the patient should be referred to the ED so one can be obtained. | CoR1, B-NR |
| 12. Patients with clinical evidence of ACS or other life-threatening causes of acute chest pain seen in the office setting should be transported urgently to the ED, ideally by EMS. | CoR1, C-LD |
| 13. In all patients who present with acute chest pain regardless of the setting, an ECG should be acquired and reviewed for STEMI within 10 minutes of arrival. | CoR1, C-LD |
| 14. In patients with chest pain in which an initial ECG is nondiagnostic, serial ECGs to detect potential ischemic changes should be performed, especially when clinical suspicion of ACS is high, symptoms are persistent, or the clinical condition deteriorates. | CoR1, C-EO |
| 15. Patients with chest pain in whom the initial ECG is consistent with an ACS should be treated according to STEMI and NSTE-ACS guidelines. | CoR1, C-EO |
| 16. In all patients presenting to the ED with acute chest pain and suspected ACS, cTn (ideally high-sensitivity) should be measured as soon as possible after presentation. | CoR1, C-LD |
| 17. In patients presenting with acute chest pain, a chest radiograph is useful to evaluate for other potential cardiac, pulmonary, and thoracic causes of symptoms. | CoR1, C-EO |
| 18. In patients presenting with acute chest pain, serial cTn I or T levels are useful to identify abnormal values and a rising or falling pattern indicative of acute myocardial injury. | CoR1, B-NR |
| 19. In patients presenting with acute chest pain, high-sensitivity cTn is the preferred biomarker because it enables more rapid detection or exclusion of myocardial injury and increases diagnostic accuracy. | CoR1, B-NR |
| 20. Clinicians should be familiar with the analytical performance and the 99th percentile upper reference limit that defines myocardial injury for the cTn assay used at their institution. | CoR1, C-EO |
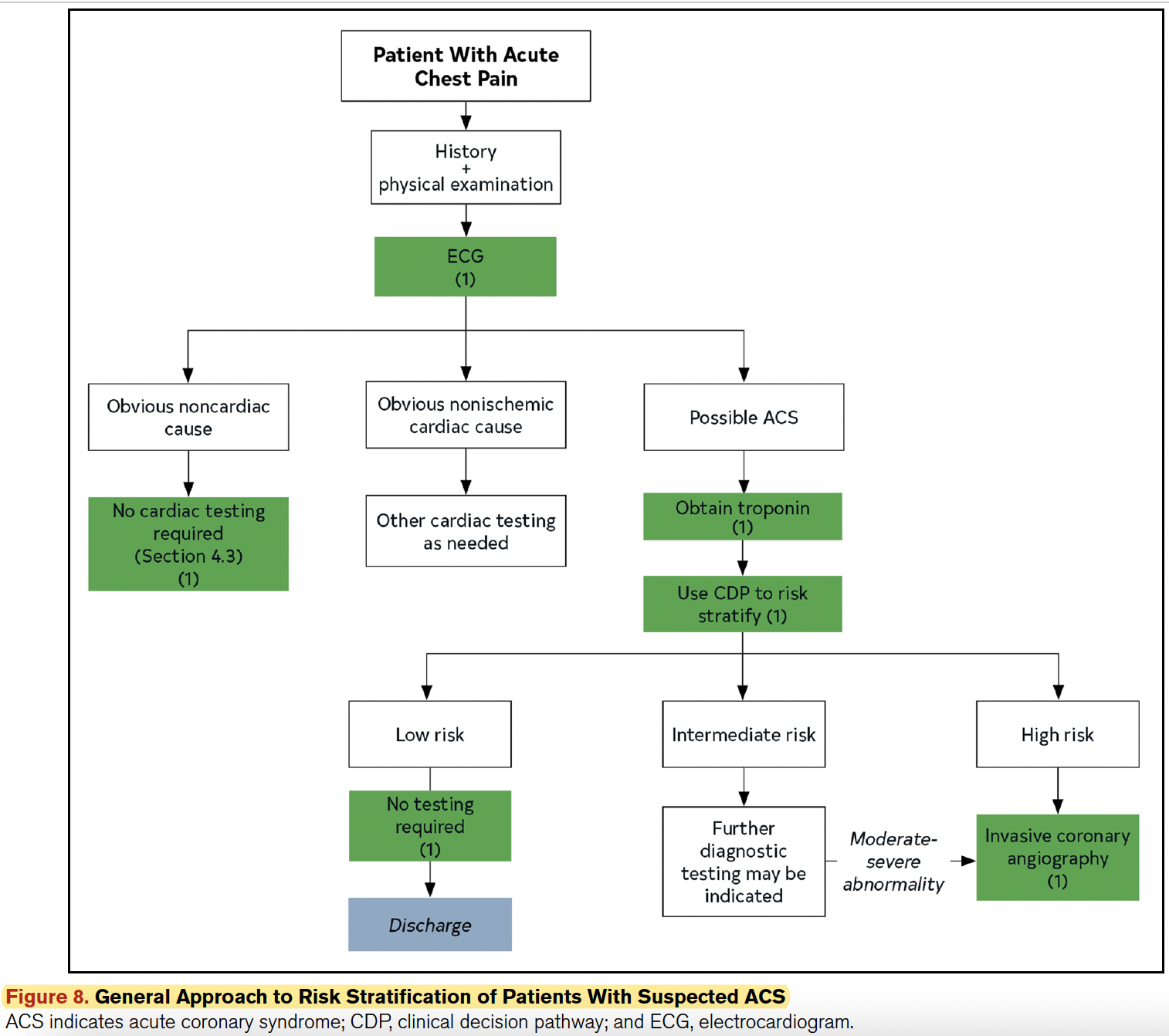
| 21. In patients presenting with acute chest pain and suspected ACS, clinical decision pathways (CDPs) should categorize patients into low-, intermediate-, and high-risk strata to facilitate disposition and subsequent diagnostic evaluation. | CoR1, B-NR |
| 22. In the evaluation of patients presenting with acute chest pain and suspected ACS for whom serial troponins are indicated to exclude myocardial injury, recommended time intervals after the initial troponin sample collection (time zero) for repeat measurements are: 1 to 3 hours for high-sensitivity troponin and 3 to 6 hours for conventional troponin assays. | CoR1, B-NR |
| 23. To standardize the detection and differentiation of myocardial injury in patients presenting with acute chest pain and suspected ACS, institutions should implement a CDP that includes a protocol for troponin sampling based on their particular assay. | CoR1, C-LD |
| 24. In patients with acute chest pain and suspected ACS, previous testing when available should be considered and incorporated into CDPs. | CoR1, C-LD |
| 25. Patients with acute chest pain and a 30-day risk of death or MACE <1% should be designated as “low risk.” | CoR1, B-NR |
| 26. For intermediate-risk patients with acute chest pain, TTE is recommended as a rapid, bedside test to establish baseline ventricular and valvular function, evaluate for wall motion abnormalities, and to assess for pericardial effusion. | CoR1, C-EO |
| 27. For intermediate-risk patients with acute chest pain and no known CAD eligible for diagnostic testing after a negative or inconclusive evaluation for ACS, CCTA is useful for exclusion of atherosclerotic plaque and obstructive CAD. | CoR1, A |
| 28. For intermediate-risk patients with acute chest pain, moderate-severe ischemia on current or prior (≤1 year) stress testing, and no know CAD established by prior anatomic testing, ICA is recommended. | CoR1, C-EO |
| 29. For intermediate-risk patients with acute chest pain and no known CAD who are eligible for cardiac testing, either exercise ECG, stress echocardiography, stress PET/SPECT MPI, or stress CMR is useful for the diagnosis of myocardial ischemia. | CoR1, B-NR |
| 30. For intermediate-risk patients with acute chest pain and no known CAD, with a coronary artery stenosis of 40% to 90% in a proximal or middle coronary artery on CCTA, FFR-CT can be useful for the diagnosis of vessel-specific ischemia and to guide decision-making regarding the use of coronary revascularization. | CoR1, B-NR |
| 31. For intermediate-risk patients with acute chest pain who have known CAD and present with new onset or worsening symptoms, GDMT* should be optimized before additional cardiac testing is performed. | CoR1, A |
| 32. For intermediate-risk patients with acute chest pain who have worsening frequency of symptoms with significant left main, proximal left anterior descending stenosis, or multivessel CAD on prior anatomic testing or history of prior coronary revascularization, ICA is recommended. | CoR1, A |
| 33. For patients with acute chest pain and suspected ACS who have new ischemic changes on electrocardiography, troponin confirmed acute myocardial injury, new onset left ventricular systolic dysfunction (ejection fraction <40%), newly diagnosed moderate-severe ischemia on stress testing, hemodynamic instability, and/or a high clinical decision pathway (CDP) risk score should be designated as “high risk” for short-term MACE. | CoR1, B-NR |
| 34. For patients with acute chest pain and suspected ACS who are designated as high risk, ICA is recommended. | CoR1, C-EO |
| 35. In patients with prior CABG surgery presenting with acute chest pain who do not have ACS, performing stress imaging is effective to evaluate for myocardial ischemia or CCTA for graft stenosis or occlusion. | CoR1, C-LD |
| 36. In patients with prior CABG surgery presenting with acute chest pain, who do not have ACS or who have an indeterminate/ nondiagnostic stress test, ICA is useful. | CoR1, C-LD |
| 37. In patients who experience acute unremitting chest pain while undergoing dialysis, transfer by EMS to an acute care setting is recommended. | CoR1, B-NR |
| 38. For patients with acute chest pain and suspected ACS who are deemed low risk by a CDP, patient decision aids are beneficial to improve understanding and effectively facilitate risk communication. | CoR1, B-R |
| 39. For patients with acute chest pain and suspected ACS who are deemed intermediate risk by a CDP, shared decision-making between the clinician and patient regarding the need for admission, for observation, discharge, or further evaluation in an outpatient setting is recommended for improving patient understanding and reducing low-value testing. | CoR1, B-R |
| 40. In patients with acute chest pain in whom other potentially life-threatening nonischemic cardiac conditions are suspected (eg. aortic pathology, pericardial effusion, endocarditis), TTE is recommended for diagnosis. | CoR1, C-EO |
| 41. In patients with acute chest pain where there is clinical concern for aortic dissection, computed tomography angiography (CTA) of the chest, abdomen, and pelvis is recommended for diagnosis and treatment planning. | CoR1, C-EO |
| 42. In patients with acute chest pain where there is clinical concern for aortic dissection, TEE or CMR should be performed to make the diagnosis (if CTA is unavailable/contraindicated). | CoR1, C-EO |
| 43. In stable patients with acute chest pain with high clinical suspicion for PE, CTA using a PE protocol is recommended. | CoR1, B-NR |
| 44. For patients with acute chest pain and possible PE, need for further testing should be guided by pretest probability. | CoR1, C-EO |
| 45. In stable patients with acute chest pain with high clinical suspicion for PE, CTA using a PE protocol is recommended. | CoR1, B-NR |
| 46. For patients with acute chest pain and possible PE, need for further testing should be guided by pretest probability. | CoR1, C-EO |
| 47. In patients with acute chest pain and myocardial injury who have nonobstructive coronary arteries on anatomic testing, CMR with gadolinium contrast is effective to distinguish myopericarditis from other causes, including myocardial infarction and nonobstructive coronary arteries (MINOCA). | CoR1, B-NR |
| 48. In patients with acute chest pain with suspected acute myopericarditis, CMR is useful if there is diagnostic uncertainty, or to determine the presence and extent of myocardial and pericardial inflammation and fibrosis. | CoR1, B-NR |
| 49. In patients with acute chest pain and suspected myopericarditis, TTE is effective to determine the presence of ventricular wall motion abnormalities, pericardial effusion, valvular abnormalities, or restrictive physiology. | CoR1, C-EO |
| 50. In patients presenting with acute chest pain with suspected or known history of VHD, TTE is useful in determining the presence, severity, and cause of VHD. | CoR1, C-EO |
| 51. In patients presenting with acute chest pain with suspected or known VHD in whom TTE diagnostic quality is inadequate, TEE (with 3D imaging if available) is useful in determining the severity and cause of VHD. | CoR1, C-EO |
| 52. Patients with acute chest pain should be evaluated for noncardiac causes if they have persistent or recurring symptoms despite a negative stress test or anatomic cardiac evaluation, or a low-risk designation by a CDP. | Cor1, C-EO |
| 53. In patients with sickle cell disease who report acute chest pain, emergency transfer by EMS to an acute care setting is recommended. | CoR1, B-NR |
| 54. For patients with stable chest pain and no known CAD presenting to the outpatient clinic, a model to estimate pretest probability of obstructive CAD is effective to identify patients at low risk for obstructive CAD and favorable prognosis in whom additional diagnostic testing can be deferred. | CoR1, B-NR |
| 55. For intermediate-high risk patients with stable chest pain and no known CAD, CCTA is effective for diagnosis of CAD, for risk stratification, and for guiding treatment decisions. | CoR1, A |
| 56. For intermediate-high risk patients with stable chest pain and no known CAD, stress imaging (stress echocardiography, PET/SPECT MPI or CMR) is effective for diagnosis of myocardial ischemia and for estimating risk of MACE. | CoR1, B-R |
| 57. In intermediate-high risk patients with stable chest pain who have pathological Q waves, symptoms or signs suggestive of heart failure, complex ventricular arrhythmias, or a heart murmur with unclear diagnosis, use of TTE is effective for diagnosis of resting left ventricular systolic and diastolic ventricular function and detection of myocardial, valvular, and pericardial abnormalities. | CoR1, B-NR |
| 58. For patients with obstructive CAD and stable chest pain, it is recommended to optimize GDMT*. | CoR1, A |
| 59. For patients with known nonobstructive CAD and stable chest pain, it is recommended to optimize preventive therapies. | CoR1, C-EO |
| 60. For patients with obstructive CAD who have stable chest pain despite GDMT and moderate/severe ischemia, ICA is recommended for guiding therapeutic decision-making. | CoR1, A |
| 61. For patients with obstructive CAD who have stable chest pain despite optimal GDMT, those referred for ICA without prior stress testing benefit from FFR or instantaneous wave free ratio. | CoR1, A |
| 62. For symptomatic patients with obstructive CAD who have stable chest pain with CCTA-defined ≥50% stenosis in the left main coronary artery, obstructive CAD with FFR with CT ≤0.80, or severe stenosis (≥70%) in all 3 main vessels, ICA is effective for guiding therapeutic decision-making. | CoR1, B-R |
| 63. For patients with obstructive CAD who have stable chest pain despite optimal GDMT, stress PET/SPECT MPI, CMR, or echocardiography is recommended for diagnosis of myocardial ischemia, estimating risk of MACE, and guiding therapeutic decision-making. | CoR1, B-NR |
| 64. In patients who have had prior CABG surgery presenting with stable chest pain whose noninvasive stress test results show moderate/severe ischemia, or in those suspected to have myocardial ischemia with indeterminate/nondiagnostic stress test, ICA is recommended for guiding therapeutic decision-making. | CoR1, C-LD |
| AGAINST Clinical Action | |
| 1. For patients with acute chest pain and suspected ACS initially evaluated in the office setting, delayed transfer to the ED for ECG, cTn or other diagnostic testing should be avoided. | Cor3, C-LD |
| 2. With availability of cTn, creatine kinase myocardial (CK-MB) isoenzyme and myoglobin are not useful for diagnosis of acute myocardial injury. | Cor3, B-NR |
*GDMT = guideline-directed medical therapy
CCTA = Coronary computerized tomography angiography. ICA = Invasive coronary angiography.
Benefits of Recommendations: The evidence reviews and recommendations presented here encompass the body of literature synthesized, and discussions amongst various experts on the guidelines panel, which include 2 EM physicians. They should lead overall optimal patient safety outcomes in the 30day period beyond the ED visit, and lead to high-value resource utilization and cost-savings.
Harms/Adverse Effects of Recommendations: There was no inclusion of patient/public stakeholders in this guidelines panel, nor was there any evidence included as to what patient values/preferences would be for the multitude of acute chest pain diagnostics, therapeutics and outcomes discussed here. This clinician-/disease-outcomes oriented approach threatens the validity of outcomes that patients may actually care about, beyond those discussed here. Furthermore, there is incomplete discussion about the harms of invasive testing, but these do not necessarily influence ED decision-making.
Barriers to Uptake: Not formally discussed. These may include access to institutional hs-cTrop tests, and advanced testing (eg. CCTA, stress tests, ICA). Very few of these CoR1 & 3 Recs are based on strong levels of evidence; there are only 7 Recs with Level A supporting evidence, few (none?) of which have a direct impact on ED care/decision-making. None of these are likely candidates for use as ED quality improvement performance metrics (which should be based on high-quality supporting evidence).
Facilitators of Uptake: Numerous clinical algorithms offered for ED adoption/ adaptation. Cost considerations are described in Section 5.3.
CLINICAL COMMENTARY: Chest pain is the 2nd most common ER chief complaint (#1 = injury) in the US (4.7% of all ED visits), with a lifetime prevalence of 20-40% (F>M). Over 50% are ultimately deemed non-cardiac, and 5.1% will confirm ACS in the ED.
- Transport: Activating 911/EMS services, especially those who can perform a prehospital ECG, can help facilitate direct transfer of STEMI patients to urgent PCI services. This should happen from community settings, or physician office settings; avoid use of personal automobiles, where detrimental outcomes have been confirmed. Delayed transfer for prompt ACS assessment/ time-dependant interventions can lead to detrimental outcomes.
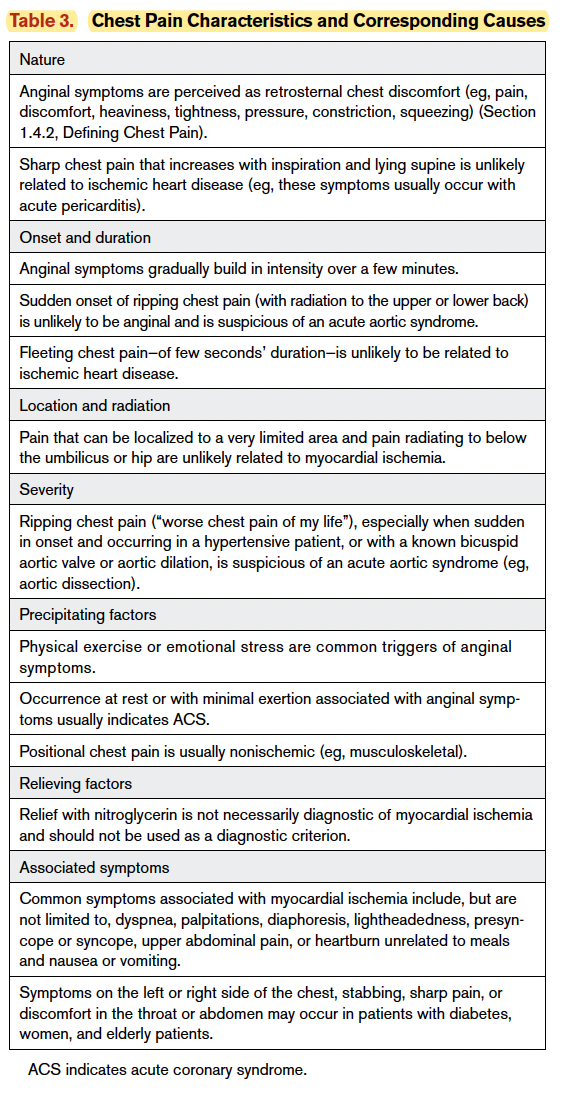
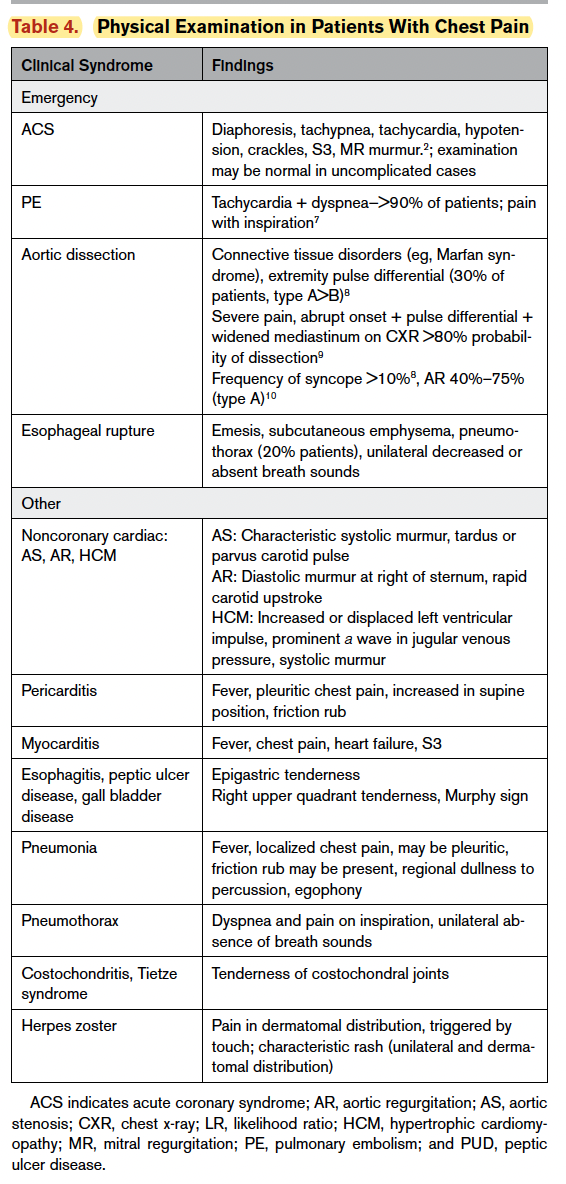
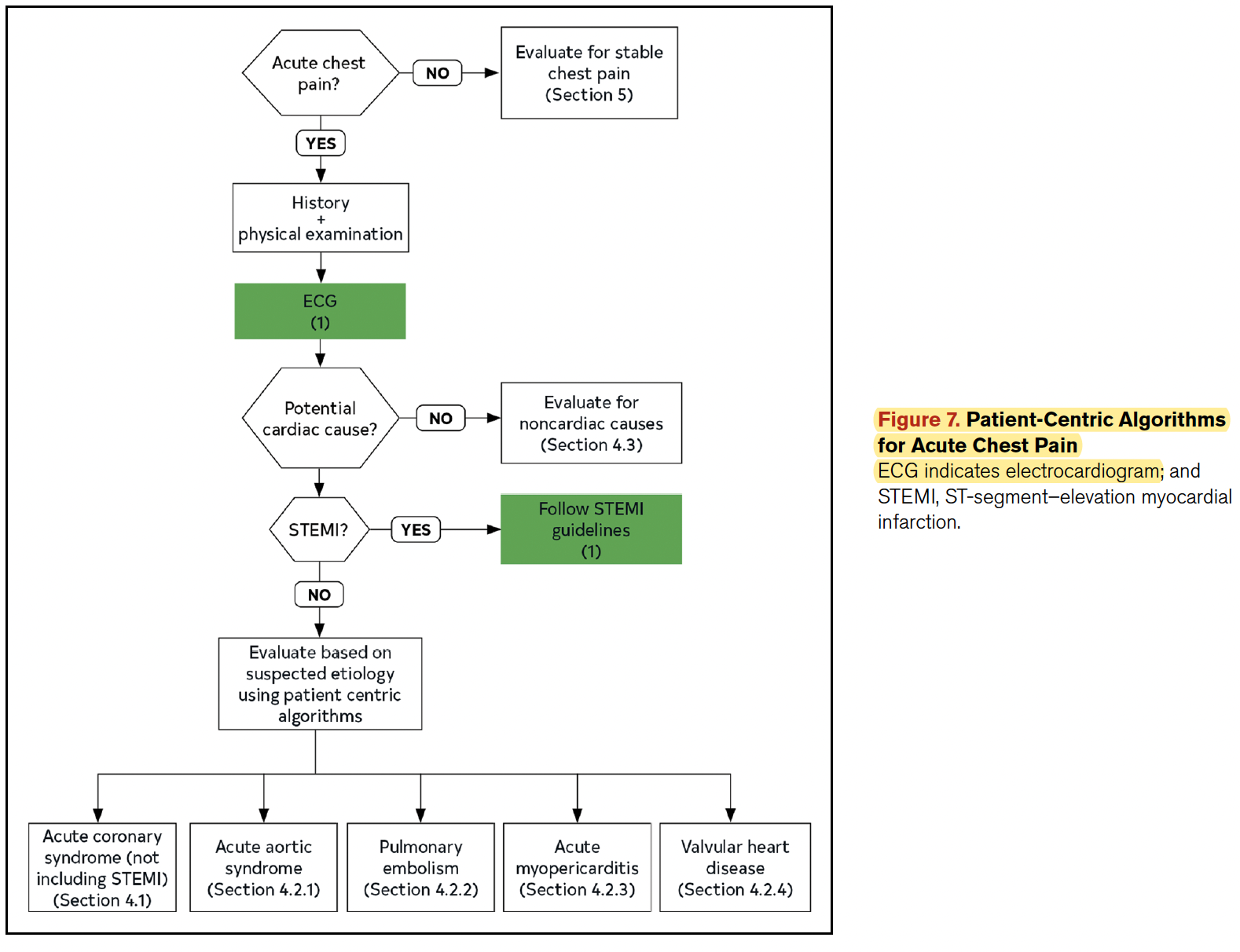
- Clinical Assessment in ED: Be mindful of “atypical” presentations in women, the elderly (age >75yo), and culturally different diasporas, especially if English is not a first language (ie. get a translator to help). Dangerous causes of chest pain include other diagnoses beyond ACS, including PE, acute aortic syndrome (see Feature CPG Jan 2021), pneumonia, pericarditis, pneumothorax, sickle cell chest crisis, and esophageal rupture. It is imperative to exclude these diagnoses, using evidence-based decision tools, in addition to confirming/excluding an ACS diagnosis. Table 3 & 4 summarize key clinical findings associated with these diagnoses. Figure 5 outlines a reasonable risk-stratified approach to ED chest pain diagnostics, and has potential to lead to reducing wasteful low-value testing. Figure 7 presents an algorithm for dangerous chest pain etiologies based on these guideline Recs, and Figure 8 presents an ACS-specific algorithm for consideration.
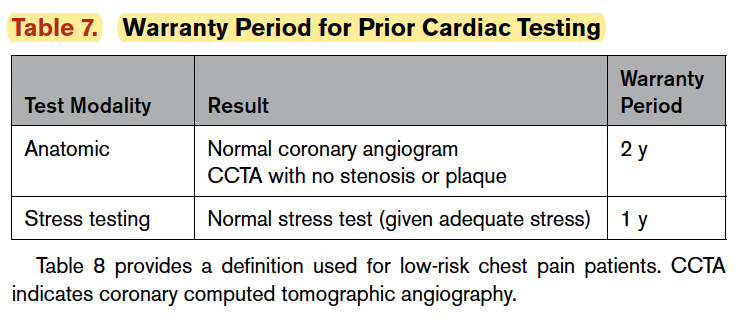
Recent cardiac testing can inform risk-stratification in the ED. For example, a normal stress test within the last year has a “warranty” of 1-year for current ACS presentation in the ED. A normal angiogram or CCTA with no stenosis/plaque has a 2yr warranty. The warranty for SPECT, however, is highly variable on the type of test used, patient’s clinical characteristics, and ejection fraction. These are summarized in Table 7.
There are unique risks for ACS in chest pain patients using cocaine and methamphetamines, but no guidance rose to the level of a CoR1 Rec. These patients should be assessed similar to other ACS patients/algorithms.
Patients at increased risk of acute aortic syndrome (dissection, hematoma, penetrating ulcer) include those with hypertension, atherosclerosis, connective tissue disorders and possible cocaine use. The annual incidence is 2-4 cases/100,000, and is characterized by an acute onset of severe chest/midback pain, often “tearing sensation” in 80-90% of cases. An excellent ED-relevant guideline has recently been published by Ohle et al (CMAJ 2020), and is the Feature CPG Summary here in January 2021.
Patients at risk of acute PE (incidence 65 cases/100,000, one third sudden death) should be risk-stratified using well-validated clinical algorithms (eg. Well’s scores, DDimers, imaging). Numerous electronic decision-aids are available online and for handheld devices that can used at the bedside.
Patients with acute myopericarditis may have sharp pleuritic chest pain, some positional changes, and possibly a pericardial friction rub. There may be widespread nonspecific ECG elevations in non-arterial distributions (transient?), and positive hs-cTrop values. Myocarditis muscle dysfunction may also present with fatigue/exercise intolerance, and heart failure symptoms. The diagnosis is confirmed with cardiac MRI, echocardiography (ED POCUS?), or cardiac CT scan. Such patients will usually be referred/admitted in the ED.
Valvular heart disease (VHD) may occur in progressive stenotic lesions (AS, MS with pulmonary HTN), or acute injury (papillary muscle injury with MR, or acute AR from aortic dissection). An urgent bedside TTE (in experienced hands) may be useful to delineate VHD causes of chest pain.
There is an extensive list of alternate diagnoses for non-cardiac chest pain, and these are summarized in Table 9. After excluding urgent/dangerous diagnoses (as above), ER physicians may consider some of the diagnoses in this list for expeditious outpatient evaluation. An acute sickle chest crisis, however, merits aggressive investigation and treatment during the ED phase, to ensure that no occult cardiac ischemia or other potentially morbid/fatal events occur.
Overall, ER physicians will need to perform some measure of pre-test probability in patients with chest pain/anginal symptoms and no prior Hx of CAD. A risk stratification scheme for such is presented in Figure 11. Knowledge of a coronary calcium score can help inform such risk assessment. Appropriate use of such tools, and negative ED hs-cTrop tests/ECGs, can streamline future referrals, admissions and invasive testing.
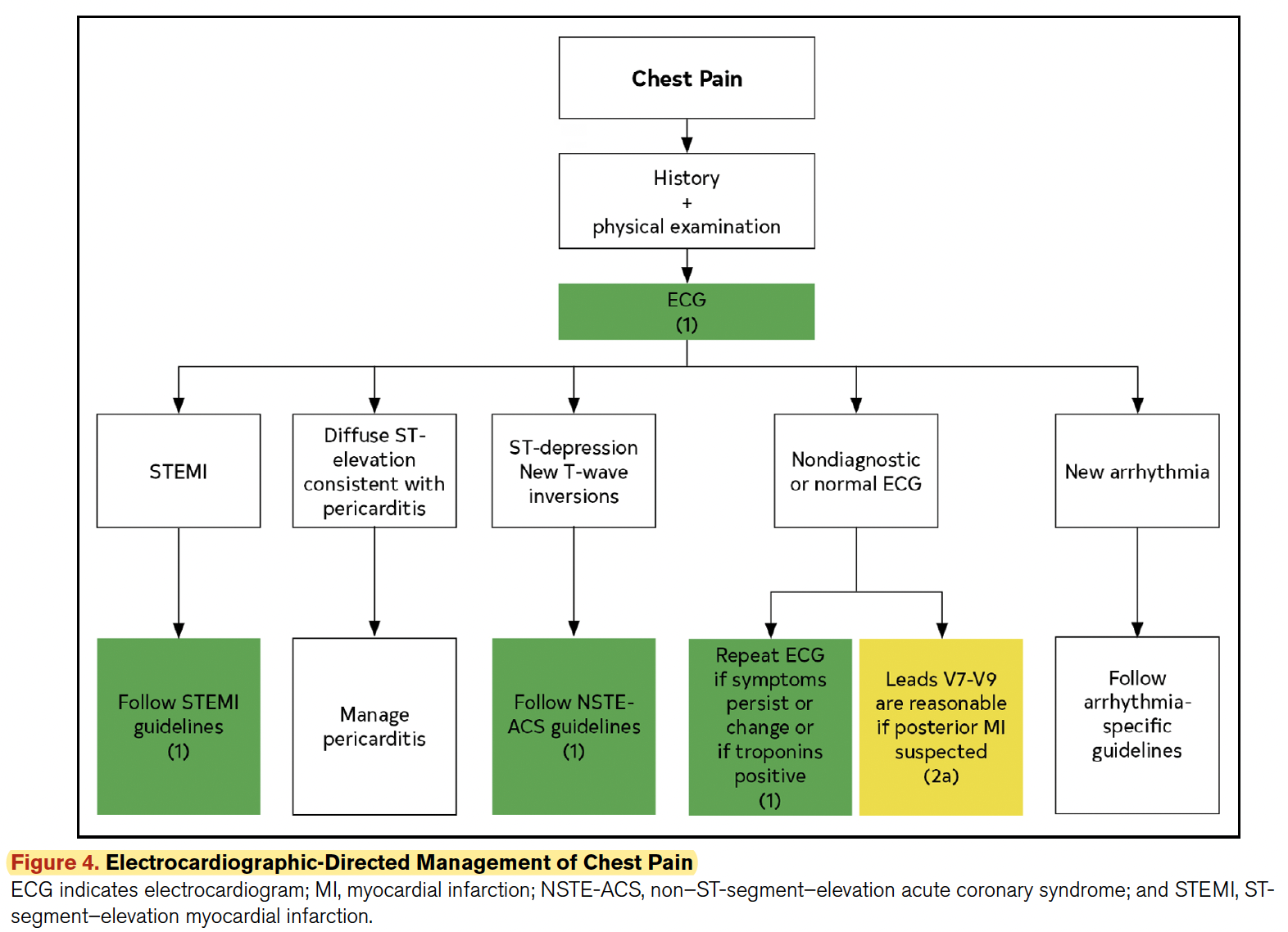
- ED Diagnostics: A rapid ECG (<10min) should identify those who may need urgent revascularization/other interventions. If an initial ECG is non-diagnostic but the clinical situation is concerning, obtain serial ECGs as warranted until a definitive decision threshold is surpassed. If indicated, make sure to get posterior and R-sided ECGs (eg. RCA or circumflex lesions). Figure 4 outlines an ECG-directed management strategy for acute chest pain. A CXR may be useful to assess non-ACS diagnoses (eg. PTX, CAP, esophageal rupture), but is usually non-contributory for ACS scenarios. High-sensitivity cardiac troponin tests, either single positive or serially positive, delta increase beyond your institutional diagnostic cutoff threshold, or serially negative (0 and 1/2/3hrs) will be useful to rule in/out ED ACS, and support disposition decisions. Be mindful that hs-cTrop thresholds may need adjustment for various modifiers (eg. gender, age, comorbidities [eg. CKD]). When hs-cTrop tests are available, avoid other less discriminatory markers (eg. CK-MB, myoglobin). There is emerging evidence that serial hs-cTrop results may out-perform “validated” risk scores (eg. TIMI, HEART); these are summarized in Table 6.
Institutional chest pain clinical decision pathways (CDPs) are highly useful, and all EDs should have/create one based on these (and similar) guidelines, in order to streamline chest pain assessment, risk stratification, high-value diagnostics/ interventions, and safe disposition. If these CDPs use various “validated” risk scores, then the summary characteristics of such pathways are listed in Table 8. Ideally such CDPs should be developed with multi-disciplinary stakeholders to ensure the most optimal uptake/engagement (eg. ED/medicine/cardiology physicians, lab medicine, nursing, diagnostic imaging?). Lab medicine partners are critical to optimize diagnostic hs-cTrop cutoffs for the institutional assays used. There are NO validated CDPs based on single tests using conventional troponin assays.
In post-CABG patients, the chest pain differential is broader, and may include the follwing: as myocardial ischemia from acute graft stenosis or occlusion, pericarditis, PE, sternal wound infection, or bony nonunion. Post-sternotomy pain syndrome is defined as discomfort after thoracic surgery, persisting for at least 2 months, and without apparent cause. The incidence of post-sternotomy pain syndrome ranges from 7-66%, with a higher prevalence in women compared with men within the first 3 months of thoracic surgery (51.4% vs 31.3%) but, after 3 months, postoperative sex difference in prevalence was not seen. For saphenous grafts, the 1yr failure rate is 10-20%, and 50% at 10yrs. Internal mammary artery (IMA) grafts, however, retain a 90-95% patency rate up to 10-15yrs post graft. Radial artery grafts also have higher patency rates at 5yrs compared to saphenous vein grafts. CCTA has excellent Dx test properties for assessing complete graft occlusion compared to ICA (Sens 99%, Spec 99%).
In CKD/dialysis patients, there is a chest pain incidence of 2-5%, and an increased risk of early atherosclerosis. Expanded CP diagnoses to consider include hemolysis, pleuritis, GERD, subclavian steal, vessel perforation from dialysis catheter, hypotension and tachyarrhythmias from electrolyte shifts. Chest pain may be a less common symptom for ACS in these patients, and may include dyspnea or diaphoresis.
For skilled/experienced users, ED POCUS/TTE can be useful to rule out other non-cardiac chest pain syndromes (eg. effusions +/- tamponade, PE with RV strain, cardiac wall/valve ruptures, masses, endocarditis). Medicolegal liability issues for ED TTE diagnosis, however, is not discussed.
For the evaluation of an acute sickle chest syndrome, the following tests are recommended: ECG, troponin test, complete bloodcount with white blood cell differential, reticulocyte count, anteroposterior and lateral chest radiograph, and blood and sputum cultures.
There is a population with suspected Ischemia and No Obstructive CAD (INOCA), due to altered microvascular flow; this is most common in women, and patients with hypertension, diabetes/insulin-resistant states, LVH or infiltrative heart disease. A care pathway for patients with suspected INOCA is presented in Figure 14.
- ED Therapeutics: Once an ACS/STEMI is identified, treat as per appropriate evidence-based practices or local care paths.
- ED Disposition: Using validated CDPs can reduce admissions by 21-43%, which leads to substantial resource savings. Low-risk patients identified through institutional ED CDPs should be referred to appropriate out-patient evaluation services where available. Post-discharge decisions can be made by appropriate physicians with patients in a shared decision-making manner.
“Intermediate” risk patients may present more of a diagnostic dilemma (not high- nor low-risk). A bedside TTE is recommended for wall motion, valvular integrity, etc., but this may require a skill/experience set that is beyond most ED physicians, and many ED physicians may not be comfortable/willing to take decision liability risks based on their ED POCUS skills. Most Recs presented here suggest more advanced testing once ED CDPs fail to rule out a “low-risk” situation. If your ED can achieve such recommendations (eg. CCTA, stress XST, ECHO, SPECT, etc.) during the index ED visit, you may proceed as appropriate. If not, then you may need to refer/admit for expedited investigations. ED CCTA, when negative, has been shown to reduce ED length of stay and subsequent testing costs in a safe manner. Figure 9 summarizes an evaluation algorithm for intermediate patients with NO known CAD. Figure 10 summarizes an approach to intermediate risk patients with known CAD, which inevitably involves advanced imaging assessments (eg. CCTA, PCA) during the index visit. Unless your ED can expedite this during the index visit, these patients likely need referral/admission for further investigations.
“High risk” patients include those with the following: new ischemic changes on the ECG, troponin-confirmed AMI, new-onset left ventricular systolic dysfunction (ejection fraction <40%), newly diagnosed moderate-severe ischemia on stress imaging, and/or a high risk score on CDP. These patients all need referral/admission for expedited angiography and aggressive risk management for otherwise high short-term MACE incidence. Approximately 6% to 15% of troponin-positive ACS occurs in the absence of obstructive CAD, but this will never be confirmed during the index ED visit.
Use of validated shared-decision making (SDM) tools can assist in risk-assessment conversations, and with ED discharge and subsequent follow-up appointments. A number of such instruments have been created and validated, most notably at Mayo Clinic (accessible at: https://carethatfits.org/chest-pain-choice/). Many of these tools have proven to increase patient knowledge, engagement, satisfaction, and reduce low-value testing in the 30day post-ED visit period.
For patients with stable chest pain and negative ED testing, ED physicians may consider the following Recs:
- Low-risk CAD: Expedited outpatient mgt. (Rec 54). See Figure 12.
- Intermediate-risk CAD and/or ED testing abnormalities: Consider CCTA, PET/SPECT, or TTE during ED visit (or refer to consultants for observation/admission). ED testing abnormalities may include pathological Q waves, symptoms or signs suggestive of heart failure, complex ventricular arrhythmias, or a heart murmur with unclear diagnosis. (Recs 55-57). Intermediate-high risk patients have modest rates of obstructive CAD (∼10%–20%) and risk of clinical events (∼1%–2% per year). CCTA is preferable in those age<65yr and not on optimal medical preventive therapies, while exercise testing is more advantageous in those >65yo, since they have a higher likelihood of obstructive CAD. Patient characteristics and existing contraindications for different testing modalities are summarized in Tables 5 & 6 (not included here).
- Known CAD and stable chest pain (Recs 59-63): Assuming negative ED testing and adequate symptom control, these patients likely need expedited investigations (to evaluate progression of obstructive CAD), possibly in an observation unit, or referral for admission. Specific investigations will be determined by past history/timing of tests, availability of testing modalities, and discussion with consultants. See Figure 13.
Prior Guideline Recommendations/Relevant Evidence:
Prior guidance suggested stress testing in low-risk ED discharged patients, but this is not recommended in this current guideline, since the risk of MACE is <1%, and expedited stress testing or cardiac imaging does NOT improve short-term outcomes. They may benefit however, from expeditious risk factor management, which can be managed as an out-patient.
These guidelines complement and significantly expand on those published by the Society of Academic Emergency Medicine Guidelines for Reasonable & Appropriate Care in the ED (SAEM-GRACE) addressing Recurrent Low-Risk Chest Pain (published July 2021; Musey PI, et al. DOI: 10.1111/acem.14296)
Areas of Evidence Gaps/Future Research Identified:
- Reducing the time from symptom onset to ED presentation/clinical evaluation, and possible use of telehealth options to reduce such times.
- Identifying and managing INOCA patients appropriately.
- Symptom classification and use in risk stratification models. Need to account for differences in gender, age, and race.
- Refining of CDPs, ideally in prospective randomized trials.
- Streamlining of low-value diagnostic testing and follow-up care in prospective randomized trials, in order to refine clinical management algorithms and decrease health care costs.
Disclaimer (if any stated): Two ER physicians represented on the authorship group: Deborah B. Diercks (SAEM representative), and Erik P. Hess (ACC/AHA).
Funding: (Reported). Funding provided by ACC/AHA. Guideline committee members volunteer their time.
Conflicts of Interested: (Reported in Supplemental Appendix materials). Many conflicts reported amongst authorship group. Voting recusals by section were reported.
CPG Quality/ Trustworthiness Standards
Amalgamated from AGREE-II/NEATS instruments.
| Quality/Trustworthiness Domain | |
| The clinical practice guideline (CPG) discloses and states explicitly its funding source. | ✔ |
| Financial conflicts of interest of guideline development group (GDG) members have been disclosed and managed. | ✔ |
| The CPG development group includes all of the relevant multidisciplinary stakeholders, including clinicians, methodologists and patients/caregivers. | ✔ |
| The CPG objectives, health questions, scope of relevant providers and target recipients of care are clearly defined. | ✔ |
| Values/preferences of patients, caregivers, advocates and/or the public with experience with the clinical disease management has been sought/integrated into CPG development (reported clearly). | X |
| The search strategy for evidence is thoroughly developed and described. | ✔ |
| The criteria for selecting relevant studies/evidence are clearly described. | ? |
| The quality, strengths and limitations of the body of evidence are clearly described (e.g., GRADE, Cochrane, etc.). Summaries of evidence tables are provided. | X |
| The health benefits, side effects, and risks were considered in formulating the recommendations. | ✔ |
| There is an explicit approach linking the evidence to formulate the recommendations. | ✔ |
| The strength of recommendations is clearly reported, including confidence in underlying evidence. | ✔ |
| Recommendations are clear and unambiguous, and easily identified in the CPG publication. | ✔ |
| Different options for management for managing the health questions are clearly presented. | ? |
| Experts externally reviewed the guideline prior to its publication. | ✔ |
| The CPG describes a procedure to update the guideline, and provides advice, tools and/or clinical pathways for easy adoption/adaptation into practice. | ✔ |
| The CPG describes barriers and facilitators to implement recommendations. | ? |
| Performance metrics for monitoring implementation of recommendations for audit/feedback have been defined appropriately. | X |
| Resource implications for implementing CPG recommendations have been discussed. | ✔ |