MONTHLY FEATURE CPG SOPR SUMMARY
CPG Citation: Pantell RH, Roberts KB, Adams WG, et al, for the Subcommittee on Febrile Infants. Pediatrics 2021; 148(2):e2021052228
Free download at: https://pediatrics.aappublications.org/content/148/2/e2021052228
**Podcast summary available at: https://thesgem.com/2021/08/sgem341-are-the-aap-guidelines-for-the-evaluation-and-management-of-the-well-appearing-febrile-infant-the-answer-to-a-never-ending-story/
Scope of Guideline: This guideline is intended for clinicians taking care of febrile infants aged 8-60days.
Included: Well-looking febrile infants (temp ≥ 38°C/100.4°F) aged 8-60days, with gestational birth age of 37-42 weeks. May also include a) Infants with resp symptoms not diagnostic of bronchiolitis, b) infectious diarrhea (get stool samples), c) presumed otitis media, d) concurrent/recent use of antibiotics, and e) positive rapid viral test results.

Excluded: Guideline not to be used with infant is not “well-appearing.” Excluded = preterm infants (<37weeks GA), infants <2weeks age with complicated perinatal course (infection/surgery), high suspicion of HSV, focal bacterial infection identified (treat as indicated), clinical bronchiolitis, documented/suspected immune compromise, congenital/chromosomal anomalies, tech intervention to sustain life, immunized within last 48hrs.
Summary download – click![]()
Key Words: Clinical practice guideline, febrile illness, infants 8-60days.
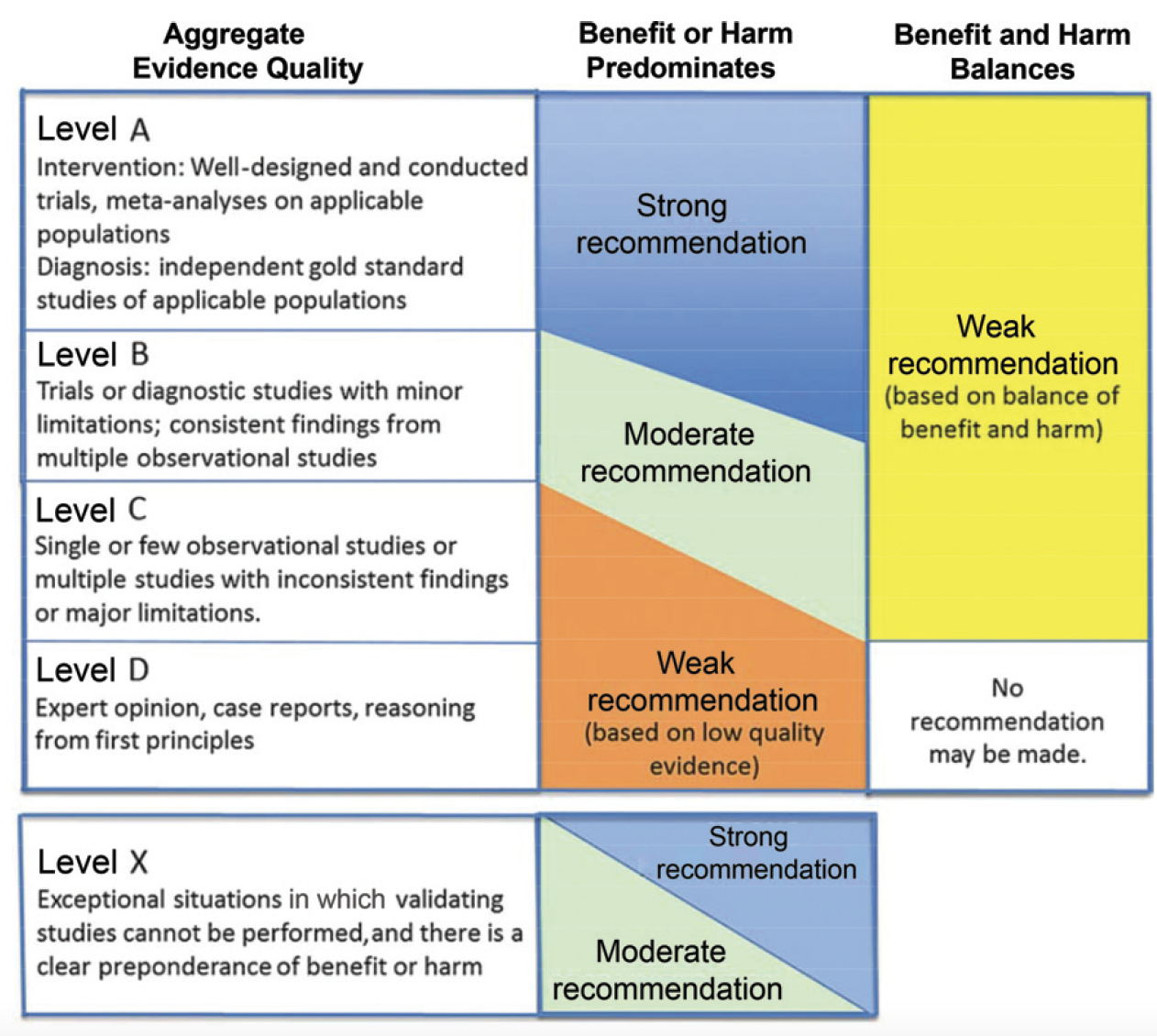
Key Action Statements (KAS): Each recommendation is accompanied by the “strength” of recommendation and the level of evidence (LoE) supporting that recommendation
| Infant Age Group | Strong | Moderate | Weak |
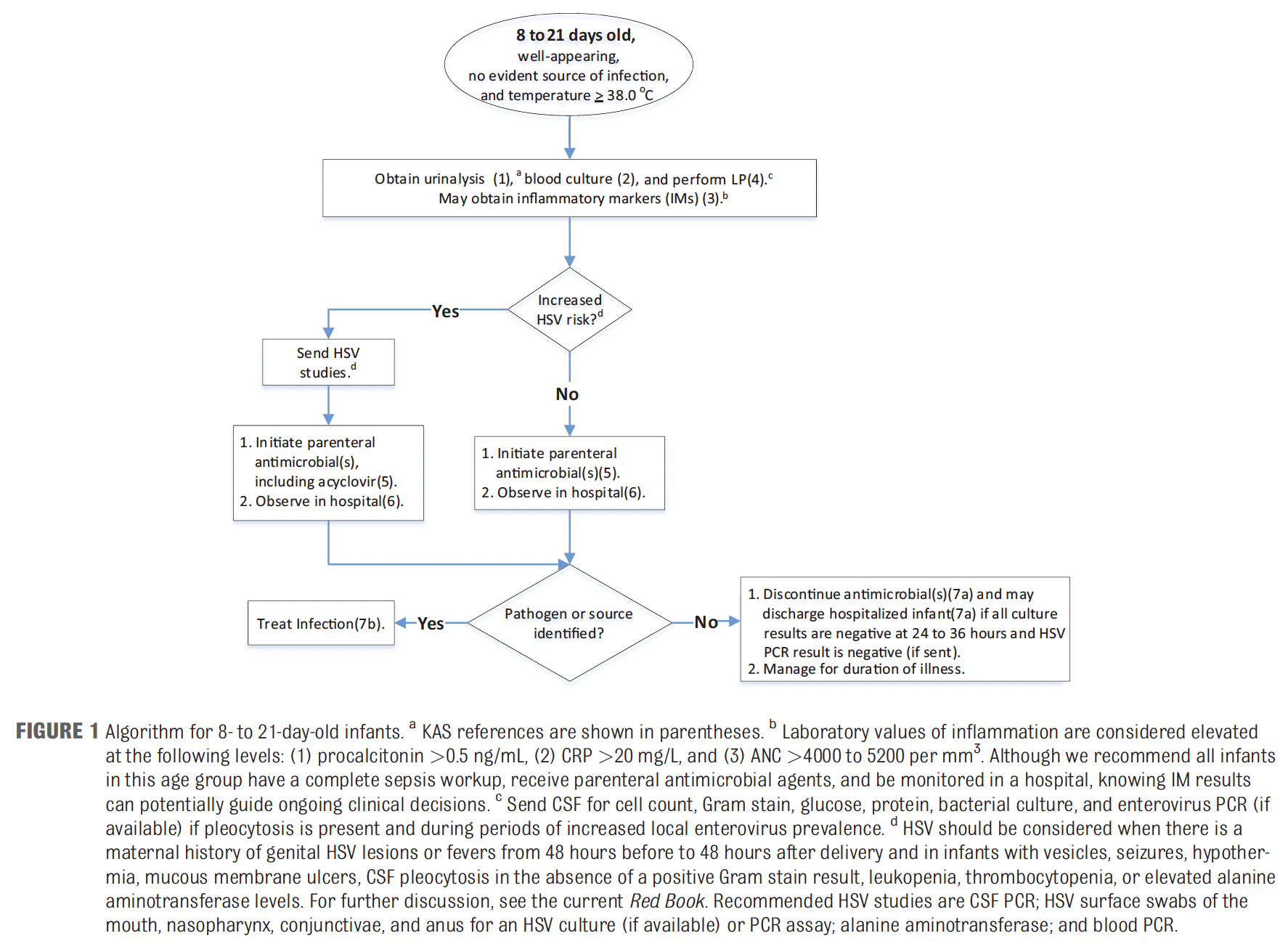
| 8-21days | KAS 1: Should obtain urine specimen by catheterization or suprapubic aspiration (SPA) of bladder for urinalysis and, if urinalysis result is positive, for culture. (A) KAS 2: Should obtain a blood culture. (A) KAS 4: Should obtain CSF for analysis (WBC, protein, glucose, Gram stain) and culture for bacteria. Assess also for HSV and enterovirus. (A) KAS 5: Should initiate parenteral antimicrobial therapy. (A) KAS 7b: Should treat infants’ positive bacterial pathogens in urine, blood, or CSF with targeted antimicrobial therapy for the duration of time consistent with the nature of the disease, responsible organism, and response of the infant to treatment. (A) | KAS 6: Should actively monitor infants while awaiting results of bacterial cultures in a hospitalsetting with nurses and staff experienced in the care of neonates/young infants. (B) KAS 7a: Should discontinue parenteral antimicrobial agents and discharge hospitalized patients when all of the following criteria are met: (1) culture results are negative for 24–36 h or only positive forcontaminants; (2) the infant continues to appear clinically well or is improving (eg, fever, feeding); (3) there no other reasons for hospitalization. (B) | KAS 3: May assess IMs. (B)IM = Inflammatory Mediators (CRP, Procalcitonin, WBC/ANC) |
| 22-28days | KAS 8: Should obtain urine specimen by catheterization or SPA of bladder for urinalysis and, if urinalysis result is positive, for culture OR should obtain urine specimen by bag, spontaneous void, or stimulated void for urinalysis and, if urinalysis result is positive, obtain a catheterization or SPA specimen for culture. (A) KAS 9: Should obtain a blood culture. (A) KAS 12a. Should administer parenteral antimicrobial therapy in a hospital if either of the following apply: (1) CSF analysis suggests bacterial meningitis; (2) urinalysis result is positive. (A) KAS 14c: Should treat infants’ positive bacterial pathogens in urine, blood, or CSF with targeted antimicrobial therapy for the duration of time consistent with the nature of the disease, responsibleorganism, and response of the infant to treatment. (A) | KAS 10: Should assess IMs. (B/Strong) KAS 11b. Should obtain CSF for analysis (WBC, protein, glucose, Gram stain), and bacterial culture if any IM obtained is positive. (B) KAS 12b. May administer parenteral antimicrobial therapy in a hospital if ALL of the following apply: (1) CSF analysis is normal; (2) urinalysis is normal; (3) Any IM obtained is abnormal. (B) KAS 12c. May administer parenteral antimicrobial therapy to hospitalized infants even if ALL of thefollowing are met: (1) urinalysis is normal; (2) no IM obtained is abnormal; (3) CSF analysis is normal or enterovirus-positive. (B/Weak) KAS 13a: May manage infants at home if all of the following criteria are met: (1) Urinalysis is normal; (2) No IM obtained is abnormal. (3) CSF analysis is normal or enterovirus-positive. (4) Verbal teaching and written instructions have been provided for monitoring throughout the period of time at home. (5) Follow-up plans for reevaluation in 24 h have been developed and are in place. (6) Plans have been developed and are in place in case of change in clinical status, including means of communication between family and providers and access to emergency medical care. (B) KAS 13b: Should hospitalize infants in a facility with nurses and staff experienced in the care of neonates/young infants when CSF is not obtained or is uninterpretable. (B/Weak) KAS 14a: Should discontinue antimicrobial agents and discharge hospitalized infants after 24 to 36 hof negative culture results if both of the following are met: (1) the infant is clinically well or improving (eg, fever, feeding); (2) there are no other reasons for hospitalization. (B/Strong) KAS 14b: Should discontinue antimicrobial agents on infants managed at home when all of the following criteria are met: (1) infant is clinically well or improving (eg, fever, feeding) at time of reassessment; (2) all culture results are negative at 24–36 h; (3) there is no other infection requiring treatment (eg, otitis media). (B/Strong) | KAS 11a: Clinicians may obtain a CSF analysis on infants 22–28 d of age even if all of the followingcriteria are met: (1) urinalysis result is negative or positive; (2) no IM obtained is abnormal; (3)blood and urine cultures have been obtained; (4) infant is hospitalized. (C/Mod) KAS 12d: Should administer parenteral antimicrobial therapy for infants who will be managed at home even if ALL of the following are met: (1) urinalysis is normal; (2) No IM obtained is abnormal; (3) CSF analysis is normal. (C/Mod) |
| 29-60days | KAS 15: Should obtain urine specimen by bag, spontaneous void, or stimulated void for urinalysis and, if urinalysis result is positive, obtain a catheterization or SPA specimen for culture, OR Should obtain urine specimen by catheterization or SPA of bladder for urinalysis and, if result ispositive, for culture. (A) KAS 19a: Should use parenteral antimicrobial therapy if CSF analysis suggests bacterial meningitis. (A) KAS 20a: Should hospitalize infants in a unit with nurses and staff experienced in the care of 29- to 60-d-old infants if CSF analysis, if obtained, is abnormal. (A) KAS 21d: Should treat infants’ positive bacterial pathogens in urine, blood, or CSF with targeted antimicrobial therapy for the duration of time consistent with the nature of the disease, responsibleorganism, and response of the infant to treatment. (A) | KAS 16: Should obtain a blood culture. (B) KAS 17: Should assess IMs. (B) KAS 18b: Need not obtain CSF for analysis and culture if all IMs obtained are normal. (B) KAS 19b: May use parenteral antimicrobial therapy if both of the following apply: (1) CSF analysis (if CSF obtained) is normal; (2) any IM obtained is abnormal. (B) KAS 19c: Should initiate oral antimicrobial therapy if all of the following apply: (1) CSF analysis (if CSF obtained) is normal; (2) urinalysis result is positive; (3) no IM obtained is abnormal. (B) KAS 19d: Need not use antimicrobial therapy while awaiting bacterial culture results if all of the following are met: (1) CSF analysis, if obtained, or normal or enterovirus-positive; (2) urinalysis result is negative; (3) no IM obtained is abnormal. (B) KAS 20b: May hospitalize infants in a unit with nurses and staff experienced in the care of 29- to 60d-old infants if any IM obtained is abnormal. (B) KAS 20c: Should manage patients at home if all of the following criteria are met: (1) CSF analysis, if CSF obtained, is normal; (2) urinalysis result is negative; (3) all IMs obtained are normal; (4) appropriate parental education has been provided; (5) follow-up plans for reevaluation in 24 h havebeen developed and are in place (6) plans have been developed and are in place in case of change in clinical status, including means of communication between family and providers and access to emergency medical care. (B) KAS 20d: May manage infants without antimicrobial treatment at home without having obtained interpretable CSF if all of the following are met: (1) urinalysis result is negative; (2) all IMs obtained are normal; (3) parents can return promptly if there is a change in infant condition and agree tofollow-up in 24 to 36 h. Infants monitored at home should be reassessed in the following 24 h. (B) KAS 21a. Should discontinue antimicrobial agents when all of the following are met: (1) all bacterial culture results are negative at 24–36 h; (2) infant is clinically well or improving (eg, fever, feeding); (3) there is no other infection requiring treatment (eg, otitis media). (B/Strong) KAS 21b: Should discharge hospitalized patients with positive urine culture (UTI) results if all of the following are met: (1) blood culture result is negative; (2) result of CSF culture, if obtained, is negative; (3) infant is clinically well or improving (eg, fever, feeding); (4) there are no other reasons for hospitalization. (B/Strong) KAS 21c: Should discontinue parenteral antibiotics (if started) and begin or continue oral antimicrobial for infants with UTIs managed at home when all of the following are met: (1) urine culture result is positive; (2) all other bacterial culture results are negative at 24–36 h; (3) infant is clinically well or improving (eg, fever, feeding). (B/Strong). | KAS 18a: May obtain CSF for analysis (WBC, differential, protein, glucose, Gram stain), culture for bacteria, and test for enterovirus when CSF pleocytosis is detected or during enterovirus season if any IM is abnormal. (C) KAS 20e: Need not treat with antimicrobial therapy if all of the following apply: (1) CSF analysis (if CSF obtained) is normal; (2) urinalysis result is negative; (3) no IM obtained is abnormal. (C/Mod) |
Benefits of Recommendations:
These recommendations, with accompanying algorithms, provide clear guidance to practitioners who care for febrile infants, and clarify “how much” investigation is needed for various age groups with documented fever.
There is clarification on what are useful markers (eg. procalcitonin, CRP) and non-useful ones (WBC, ANC, bands). Although viral testing can help distinguish viral vs. bacterial etiologies, a positive viral test may not preclude a concomitant bacterial illness, or shorten hospital LOS.
The methodology used in this guideline process are strong, and meets nearly all key NEATS criteria for guideline trustworthiness (Jue et al, 2019); the only exception is the lack of parent/ caregiver stakeholders in this undertaking.
Harms/Adverse Effects of Recommendations:
There were no parents/caregivers with reported involvement in the evidence reviews or formulating recommendations for this guideline, which risks missing important parental values/preferences/priorities which should always be integral for creating trustworthy guidelines.
Certain procedures are more invasive (eg. lumbar puncture, regular/supra-pubic urine catheter) which may cause pain, trauma and concern for parents. Furthermore, various physicians may be unskilled/inexperienced/uncomfortable providing such procedures. Using non-catheter urine samples for culture can lead to unacceptably high contamination rates (false positives). False positives, in turn, lead to unnecessary antibiotic exposures, with attendant harms of same.
Antibiotic stewardship is, in general, a desirable goal in all populations, including febrile infants. Judicious decision-making, with ideally targeted antibiotic treatment based on local antibiograms (or the AAP Red Book), should be used to optimize stewardship. Routine Abx are warranted in infants <28days, given the high risk of bacteremia with subsequent morbidity/mortality. In higher age groups, Abx usage may be based on test results or other clinical parameters. Once various test/culture results are available, Abx usage should be modified/discontinued as warranted.
Prior Guideline Recommendations/Relevant Evidence:
Historical CDRs for febrile infants do not always accurately risk-stratify high vs low-risk infants for SBI, and there is abundant evidence that physicians do not reliably follow such rules anyway. A lot of unnecessary care is generated from non-adherence to CPG recommendations, and this leads to considerable differences in costs.
The rate of bacteremia drops substantially in early weeks of life (eg. week 2 = 5.3%, week 3 = 3.3%, week 4 = 1.6%; no differences by week 5 & 6); Figure 4 of CPG publication.
Barriers to Uptake: There is a need to define quality improvement performance metrics that can be used in QI intiatives; these should be limited to STRONG recommendations only that are easily measurable (eg. administrative/EMR data, not chart reviews).
It is possible that various inflammatory markers (eg. procalcitonin) may not be readily available in various ED settings.
A variety of current CDRs have a “clinical appearance” (well vs ill) criterion, which is subjective, and therefore maybe not reliable/reproducible. Different levels of experience/ judgment may influence comfort level in assessing “sick vs not sick” looking infants.
The term “SBI” (serious bacterial illness) should be retired for more specific labels: meningitis, UTI, bacteremia.
Facilitators of Uptake: Clinical algorithms are provided for ready adoption/adaptation into ED workplace.
A purposeful dialogue with families/parents re: invasive procedures (urinary catheters, lumbar puncture), and home vs. in-patient monitoring should lead to more meaningful shared decision-making (no tools provided). It will likely be the case that the “risk tolerance” of different stakeholders (physicians, families/parents) may be different, so a mutually agreeable solution for such discussions should be reached; this was evident also with different CPG panelists when formulating Key Action Statements.
CLINICAL COMMENTARY:
- UTI (E. Coli) is the most common of febrile bacteremia/meningitis in infants age 1-60days; this likely reflects treatement/vaccine protections from GBS, S. Pneumo, H. Influenza B and N. meningitidis in past years.
- Clinical observation (eg. Yale Observation Score) is not always reliable for clinical appearance.
- Positive ED viral positive tests do not necessarily exclude serious bacterial illnesses.
- Empiric antimicrobial Rx should be guided by local microbiological data.
- There are many future research questions (n=17 listed) that need to be examined in order to refine further febrile illness risk-stratification tools, investigations and management algorithms.
Disclaimer (if any stated): 3 subcommittee members had some commercial/industry disclosures. No members of the writing committee had reported conflicts.
Funding reported: None (reported)
Grading System Used: AAP Rating of Evidence/Recommendations Framework
Institute of Medicine 2011 Trustworthiness Standards
| Rating Domain | Rating (Good/Fair/Poor) |
| Establishing transparency | Good |
| Managing conflict of interest in CPG development group | Good |
| Group composition (range of stakeholders involved) | Fair (no parent/caregiver involvement) |
| Critical evaluation of supporting evidence | Good; published separately at Hui C, Neto G, Tsertsvadze A, et al. Diagnosis and management of febrile infants (0-3 months). Evid Rep Technol Assess (Full Rep). 2012;205(205):1–297. |
| Framing recommendations based on supporting evidence | Good |
| Clear articulation of recommendations | Good |
| External review by relevant stakeholders/ organizations | Good |
| Updating schedule | Good |
| Implementation issues | Good (algorithms provided) |
Supporting Systematic Review: Downloadable at: Hui C, Neto G, Tsertsvadze A, et al. Diagnosis and management of febrile infants (0-3 months). Evid Rep Technol Assess (Full Rep). 2012;205(205):1–297.