MONTHLY FEATURE CPG SOPR SUMMARY
CPG Citation: Shaker MS, Wallace DV, Golden DBK, Oppenheimer J, Bernstein JA, Campbell RL, Dinakar C, Ellis A, Greenhawt M, Khan DA, Lang DM, Lang ES, Lieberman JA, Portnoy J, Rank MA< Stukus DR, Wang J. Anaphylaxis – a 2020 practice parameter update, systematic review, and Grading of Recommendations, Assessment, Development and Evaluation (GRADE) analysis. J Allergy Clin Immunol 2020; 145(4): 1082-1123.
Downloadable at: https://doi.org/10.1016/j.jaci.2020.01.017.
PMID: 32001253
Scope of Guideline: Not specified.
Inclusion: Not clearly specified; recommendations relevant for EM practice.
Exclusion: Not clearly specified
Key Words: anaphylaxis, epinephrine, antihistamines, glucocorticoids
Special thanks to Dr.
Judy Morris (Univ of
Montreal) for expert
comments!!

Summary download – click![]()
EM-Relevant Questions Addressed in Guideline:
Q1. What risk factors should clinicians take into consideration in determining the likelihood of biphasic anaphylaxis?
Q2. Should antihistamines and/or glucocorticoids be used to prevent biphasic anaphylaxis?
Q3. Should antihistamine and/or glucocorticoid premedication be used to prevent recurrent HSRs to RCM?
Key Recommendations: Each recommendation is accompanied by the “strength” of recommendation and the level of evidence (LoE) supporting that recommendation
| Recommendations | Strength, LoE |
| FOR Clinical Action Rec1a: We suggest that a clinician incorporate severity of anaphylaxis presentation and/or the administration of >1 dose of epinephrine for the treatment of initial anaphylaxis as a guide to determining a patient’s risk for developing biphasic anaphylaxis. Rec1b: We suggest extended clinical observation in a setting capable of managing anaphylaxis (to detect a biphasic reaction) for patients with resolved severe anaphylaxis and/or those who need >1 dose of epinephrine. | Conditional, Very Low Conditional, Very Low |
| NEUTRAL Clinical Action N/A | |
| AGAINST Clinical Action Rec2: We suggest against administering glucocorticoids or antihistamines as an intervention to prevent biphasic anaphylaxis. Rec3: We suggest against routinely administering glucocorticoids and/or antihistamines to prevent anaphylaxis in patients with prior radiocontrast HSRs when readministration of a low- or iso-osmolar, nonionic RCM agent is required. | Conditional, Very Low Conditional, Very Low |
Additional Good Practice Statements
GPS1: Administer epinephrine as the first-line pharmacotherapy for uniphasic and/or biphasic anaphylaxis.
GPS2: Do not delay the administration of epinephrine for anaphylaxis, as doing so may be associated with higher morbidity and mortality.
GPS3: After diagnosis and treatment of anaphylaxis, all patients should be kept under observation in a setting capable of managing anaphylaxis until symptoms have fully resolved.
GPS4: All patients with anaphylaxis should receive education on anaphylaxis, including avoidance of identified triggers, presenting signs and symptoms, biphasic anaphylaxis, treatment with epinephrine, and the use of epinephrine auto-injectors, and they should be referred to an allergist.
CLINICAL COMMENTARY:
The lifetime prevalence of anaphylaxis is 1.6-5.1%, but fatality is rare (0.25-0.33% of ED/hospitalized cases).
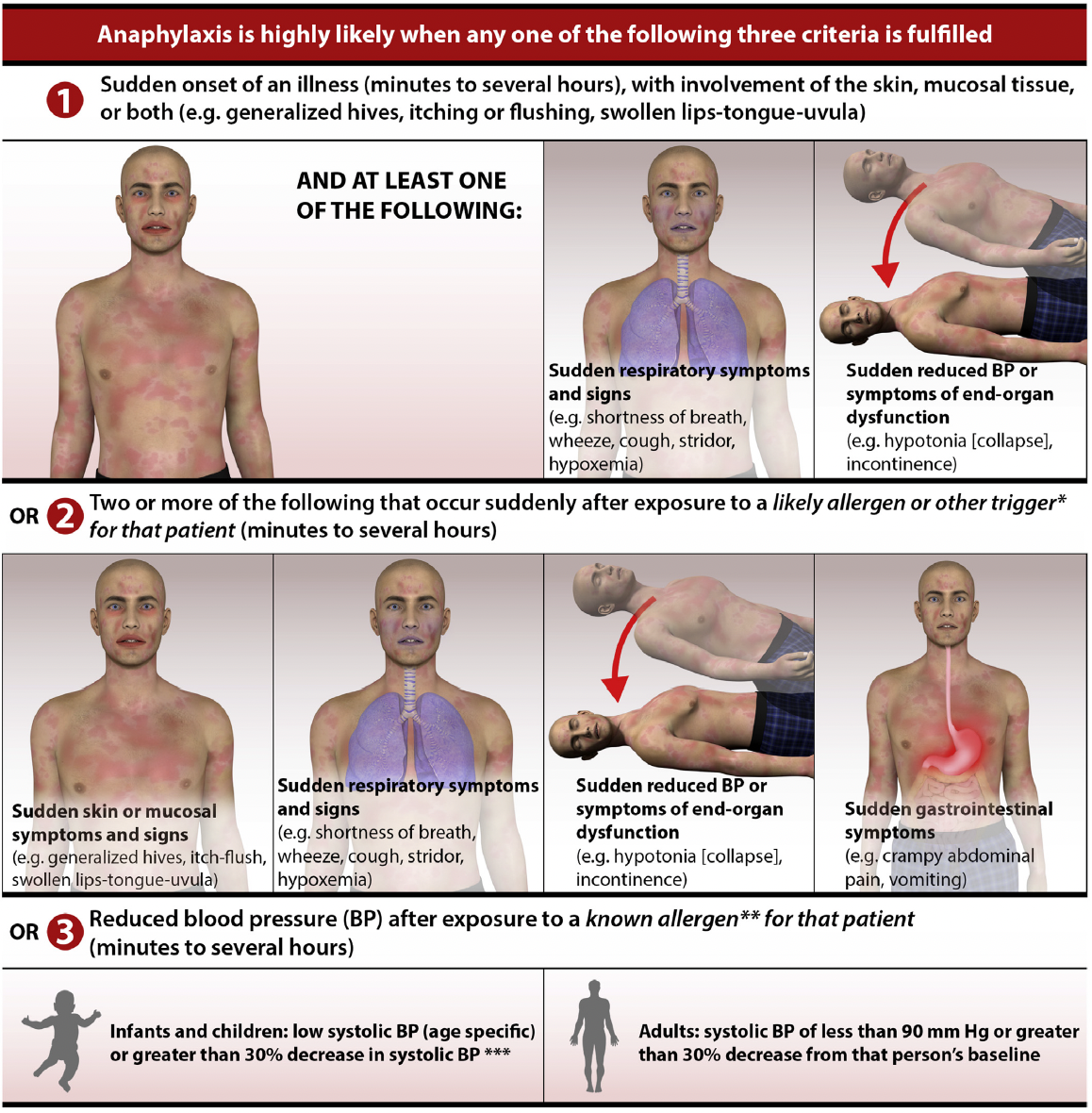
The NIAID diagnostic criteria for anaphylaxis has 95% sensitivity and 71% specificity (LR+ 3.26, LR- 0.07) in ED settings. Even ED patients who have resolved anaphylaxis symptoms (Figure) who do not require epinephrine should still receive the proper diagnosis.
Biphasic anaphylaxis (BA) occurs in 1-20% of patients, which may occur from 1-72hrs after initial attack, but has been reported up to 78hrs. Risk factors for severe anaphylaxis include the following: older age, asthma Hx, and comorbid CV/other diseases.
It is not clear what the optimal length of ED observation should be after initial anaphylaxis treatment to avoid biphasic reactions, but summary literature suggests that the range should be 1-5hrs (NPV range 95-97.3%). In a 2021 review by Simard et al (CJEM 2021), they identified slightly different risk factors for BA, including the following :
- initial anaphylaxis severity
- need for multiple epinephrine initial doses
- delay in initial epinephrine dose
- Hx of prior anaphylaxis
- unknown triggers
- young age (this is contrary to the Shaker review where older age is potentially a BA risk?)
Simard D, Bouchard V, Plourde A, et al. Factors influencing emergency department observation time following anaphylaxis: a systematic review. Can J Emerg Med 2021; 23: 480-493. DOI: 10.1007/s43678-021-00112-z
Prior Guideline Recommendations/Relevant Evidence:
A more recent anaphylaxis CPG has been published, using GRADE ADOLOPMENT methods:
Dodd A, Hughes A, Sargant N, Whyte AF, Soar J, Turner PJ. Evidence update for the treatment of anaphylaxis. Resuscitation 2021; 86-96. https://doi.org/10.1016/j.resuscitation.2021.04.010. PMID: 33895231
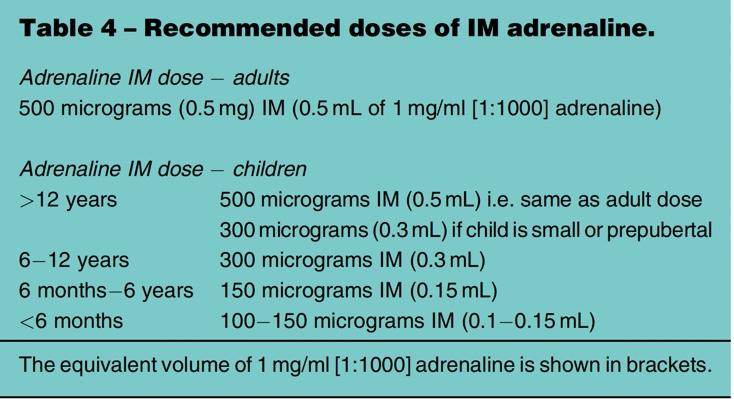
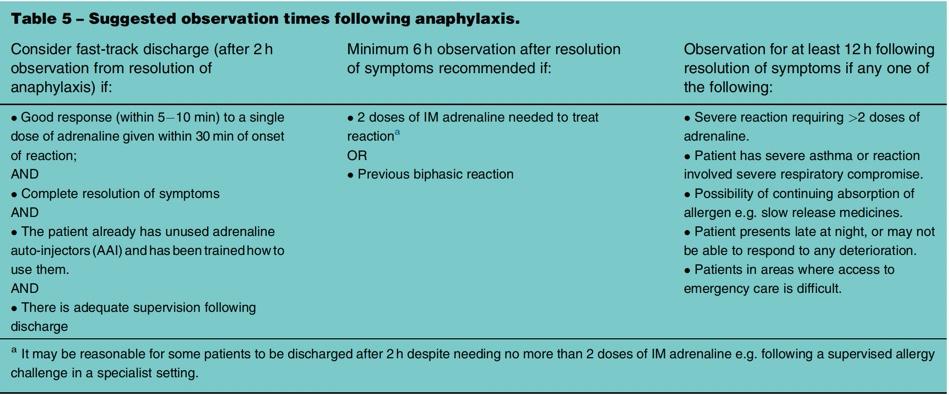
The EM-relevant recommendations are as below:
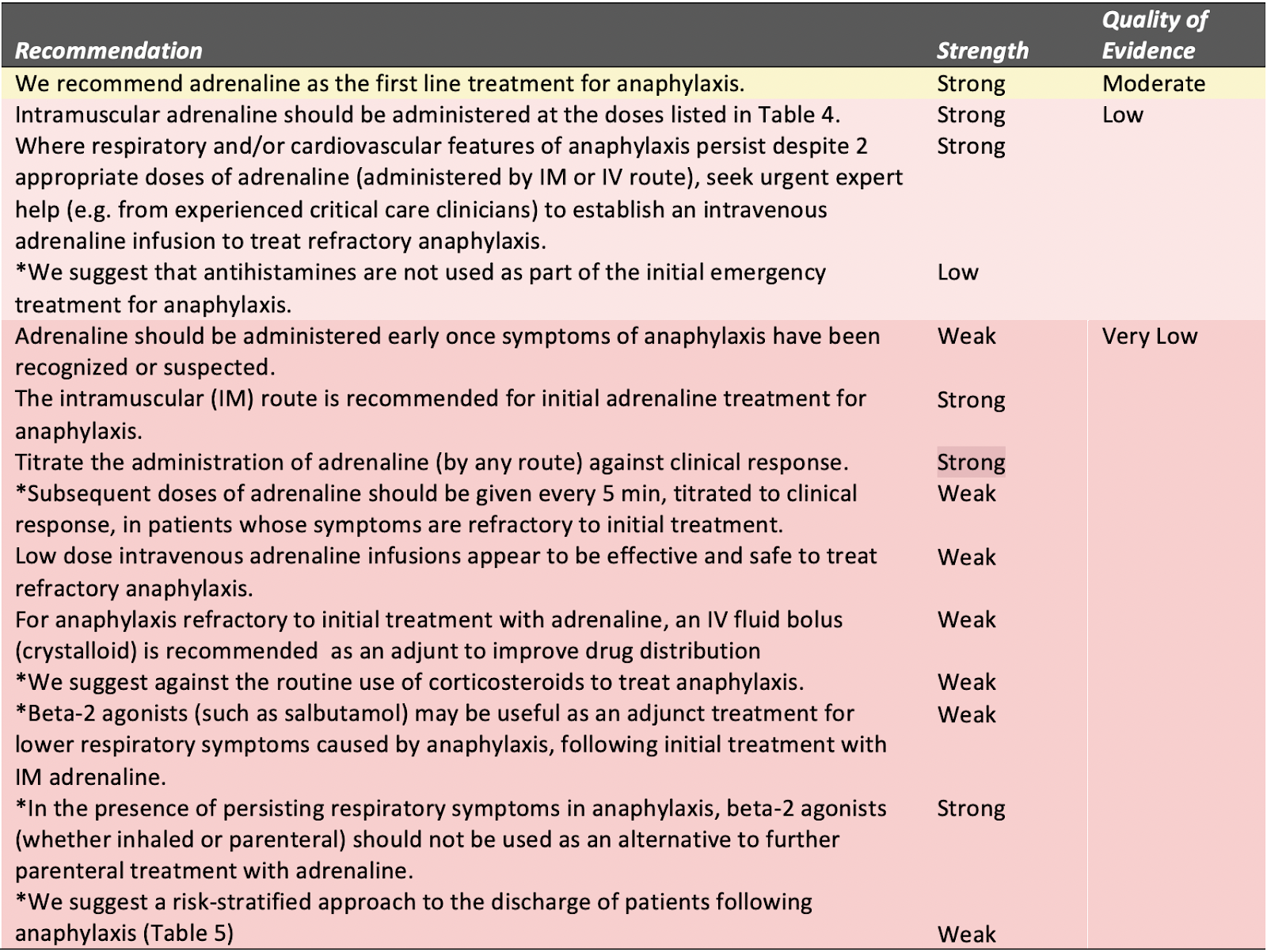
*Updated for 2021
Disclaimer (if stated): Many industry relationships with authors declared.
Funding reported: Not specified.
Grading System Used: GRADE
IOM Guideline “Trustworthiness” Checklist
| Rating Domain | Rating (Good/Fair/Poor) |
| Establishing transparency | Good |
| Managing conflict of interest in CPG development group | Fair |
| Group composition (range of stakeholders involved) | Good |
| Critical evaluation of supporting evidence | Good |
| Framing recommendations based on supporting evidence | Good |
| Clear articulation of recommendations | Good |
| External review by relevant stakeholders/organizations | Good |
| Updating schedule | Poor |
| Implementation issues | Fair |